

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The intensive care unit (ICU) is a complex organization that comprises a diverse group of health care professionals who work to serve the needs of critically ill patients. ICU care demands everyday medical decision making, which is founded on values-based attitudes, behaviors, and actions, involving various ICU caregivers (1, 2, 3). Evidence has suggested that ethical issues or conflicts are common and harmful in ICU care (4, 5). Previous studies investigating the prevalence of ethical issues focused on both nurses and physicians (6, 7, 8). Although they are part of the same team and pursue the same overall goal of care, nurses and physicians may have different views of ethical issues, such as end-of-life (EOL) care and decisions about life-sustaining treatment (LST) (9, 10). Critical care nurses, who spend the greatest amount of time with patients and families, play an important role in balancing and integrating the needs of ICU caregivers (11, 12). In this process, nurses frequently encounter many sources of ethical conflict. Unresolved ethical conflicts not only create job dissatisfaction, but may also trigger burnout syndrome in nurses (5). In order to enhance clinical outcome, a critical care team should monitor the sources and frequency of ethical issues in everyday clinical practice that are recognized by critical care nurses.
Korea has been changing social and political circumstances in ICU care environments. In the early 2000s of Korea, the delivery of appropriate critical care suffered from a shortage of full-time critical care physicians and qualified nurses, and inadequate reimbursement of medical expenses by the exclusive national insurance agency (13). During the last decade, there have been continuous efforts to improve the ICU care environment in Korea, including formulation of a certified critical care subspecialty in 2009 and classification of ICU grades for better reimbursement. Moreover, EOL care has been emerged as a big social issue in Korea, for which consensus guidelines for the withdrawal of LST were introduced in 2009 (14, 15). During this 10 yr period, ethical sensitivity about EOL care and ICU staffing was also enhanced in the studied hospital. Because one year prospective survey on ethical issues perceived by critical care nurses was performed by us in 2002, it was a good opportunity for us to study how these changes surrounding ICU care environment could be reflected in ethical issues perceived by ICU nurses. We hypothesized that enhanced ethical sensitivity about EOL care in our medical and public societies may reduce the ethical conflict related to EOL care. We thought that improved ICU staffing might reduce the frequency of ethical issues experienced by critical care nurses. For these reasons, the present study aimed to investigate the changes in ethical issues perceived by critical care nurses over the past 10 yr in ICUs of a single tertiary university-affiliated hospital in Korea, which has been continuously pursuing better improvements in critical care.
MATERIALS AND METHODS
Study design
We conducted a retrospective analysis of data obtained by prospective questionnaire surveys of critical care nurses in ICUs of a tertiary university-affiliated hospital in Korea. Data were collected prospectively during two different periods: February 1, 2002-January 31, 2003 (Period 1) and August 1, 2011-July 31, 2012 (Period 2). In Period 1, the questionnaire survey was started in the medical (M) and surgical (S) ICUs, and the neurological (NR) and neurosurgical (NS) ICUs were included 3 months later. In Period 2, we added the cardiac surgical (CS) ICU and coronary care unit (CCU), enrolling six types of ICUs from the start of the survey period.
Before the study started, critical care nurses participating in the study were educated by a trained intensivist in medical ethics through 2 hr of systematic instruction on the predefined ethical contents of the questionnaire and the objectives of the survey during Periods 1 and 2. To improve the nurses' degree of understanding regarding concepts and perceptions of ethical issues, they received e-learning programs on nursing ethics and repeated the above-mentioned study education by two intensivists in the middle of the study in Period 2.
When the nurses encountered the ethical issues, they were asked to classify their observations according to one or more topics (per case) described in the questionnaire. Open-ended questions also encouraged them to describe the experience regarding ethical issues and express their thoughts and feelings freely about their observations. The ethical issues were collected on a daily basis by a dedicated research nurse in Period 1 and an intensivist in Period 2. Collection and processing of completed questionnaire was done anonymously. Three consultants with expertise in clinical medical ethics independently and systematically reviewed and reclassified the issues that were identified. When the issue could not be classified into just one category, it was counted as an individual issue in the relevant category, and designated as a mixed issue.
Questionnaire and definition of ethical issues
The questionnaire included 27 items including the patients' demographic information, level of therapeutic intervention, the nature of nurse-identified ethical issues or conflicts, the personnel involved in ethical issues, and context of the situation. Generally, ethical issues occur when there is a conflict of values between individuals, or within individuals, concerning which of the possible options should be chosen. The ICU environment is stress prone condition and difficult ethical issues emerge between those who are involved in the cares of critically ill patients. We reviewed the available literature on investigating ethical issues or conflicts in the ICU setting. Common ethical issues include clinical problems about EOL care involving complex decisions about LST such as futility, withholding/withdrawal and do-not-resuscitate (DNR) (7, 8, 16). As well as EOL care issues, Azoulay et al. (6) indicated that ethical issues in the ICU were also mainly related to general behavior including communication gap, mistrust and inappropriate behaviors of ICU caregivers. Moreover, previous qualitative studies highlighted communication, hierarchical problems among ICU caregivers, and social problems as one of the most frequent ethical issues encountered by ICU caregivers (17, 18, 19). From these considerations, ethical issues or conflicts contained all perceived issues. This included behavior-related issues by ICU caregivers; issues regarding LST including futility, withholding/withdrawal and DNR; issues related to informed consent; resource allocation; transportation of the patient within or between hospitals; organ transplantation; medical insurance reimbursement; rebate or gifts from the patient, family or corporations; and clinical research in the ICU. In this study, behavior-related issues by ICU caregivers included inappropriate behavior of healthcare professional or the patient's family, and communication gaps among ICU caregivers. Table 1 shows the definitions of the behavior-related issues used in the study.
Environmental changes in all studied ICUs between Period 1 and 2
Table 2 shows the changes in care pattern of each ICU in studied hospital during Periods 1 and 2. MICU was a closed ICU, while the others were open ICUs. ICU nurse to bed ratio decreased from 1:2.1 in Period 1 to 1:2.0 in Period 2. MICUs and SICUs physician staffing patterns were enhanced in Period 2. Two full-time attending critical care physicians, three full-time critical care fellows, and two monthly rotating residents were more added to MICU during the last decade. SICU was additionally staffed with one full-time surgical critical care physician, one full-time critical care fellow, and two monthly rotating residents and interns. There were no full-time intensivists in the other studied ICUs. The number of beds decreased in NSICU (from 16 to 14) and NRICU (from 14 to 13). One resident was added to NRICU, but there was no change in resident or intern numbers in NSICU in the last decade. Electronic medical record system and medical emergency team have been introduced during the 10 yr between each period. Other circumstances including the in-house policy about decision making process among ICU caregivers, overall residency training policy and program have not been much altered in studied ICUs over a decade.
Statistical analysis
Data were analyzed using SPSS version 20.0 for Windows (SPSS Inc., Chicago, IL, USA). For continuous variables, a student t-test or Mann-Whitney nonparametric U-test was used for comparison between groups. A chi-square (χ2) or Fisher's exact test was used to compare the categorical variables. All nominal variables were expressed as frequencies and all continuous variables were expressed as means±standard deviation, if normally distributed. Differences were considered to be statistically significant if the P value was <0.05.
RESULTS
Cases with reported ethical issues in Period 1 and 2
The overall incidence of ethical issues identified by ICU nurses in Period 1 was represented by 89 cases (2.1%) with 101 ethical issues of 4,291 total ICU admissions (Table 3). Thirty-three ethical issues out of 915 total ICU admissions were reported in MICU (3.6%), and 22 cases of 1,733 ICU admissions (1.3%), 21 of 883 (2.4%), and 13 of 760 (1.7%) were perceived by ICU nurses in SICU, NSICU, and NRICU, respectively, in Period 1. In comparison, in Period 2, 51 cases (0.5%) with 56 ethical issues were identified among 9,302 ICU admissions. In Period 2, nurses in MICU experienced 23 cases with ethical issues out of 1,087 ICU admissions (2.1%), 16 cases in SICU out of 1,819 ICU admissions (0.9%), 5 in NSICU of 1,745 (0.3%), one in NRICU of 1,420 (0.1%), four in CSICU of 1,351 (0.3%), and two in CCU of 1,880 (0.1%). During Period 1, two cases were involved in three ethical issues, and eight cases were involved in two ethical issues, and five cases were involved in two ethical issues during Period 2.
As such, the overall incidence of reported cases with ethical issues was significantly decreased in Period 2 compared with in Period 1 (P<0.001). In both Periods, MICU showed the highest incidence of cases involving ethical issues.
Differences in the proportions of identified ethical issues between Period 1 and 2
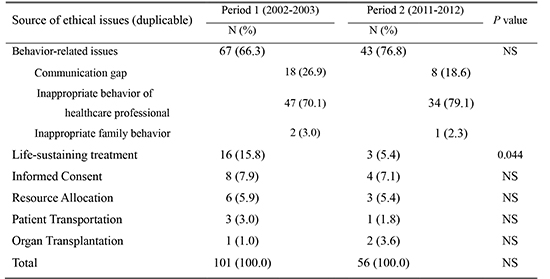
Table 4 demonstrates the changes in the reasons for ethical issues during the 10-yr period. In Period 1, behavior-related issues (n=67, 66.3%) were most frequently reported by ICU nurses, followed by LST (n=16, 13.4%) and informed consent related issues (n=8, 7.9%). The remaining ethical issues identified by ICU nurses were as follows: ethical issues related to resource allocation (n=6, 5.9%), patient transportation (n=3, 3.0%), and organ transplantation (n=1, 1.0%). In Period 2, behavior-related issues were also the leading cause of ethical issues (n=43, 76.8%). However, a significant decrease in the proportion of overall ethical issues was observed in those concerning LST in Period 2 compared with Period 1 (3 [5.4%] and 16 [15.8%], respectively; P=0.044). In Period 2, there was no significant difference in the other ethical issues regarding their proportion between Period 1 and 2.
Behavior-related issues in Period 1 and 2
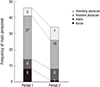
Inappropriate healthcare professional behavior was the most frequent behavior-related issue in both Periods (47 of 67, 70.1% in Period 1 vs. 34 of 43, 79.1% in Period 2; Table 4). In Period 1, physicians were involved in 38 (82.6%) of the reported cases (Fig. 1). Of all the physicians, residents were the most frequently involved (27 cases, 58.7%), followed by interns (6, 13%) and attending physicians (5, 10.9%). Nurses involved eight cases (17.4%). In Period 2, most personnel involved in behavior-related issues were physicians. Again, resident physicians were the personnel most frequently involved (18, 52.9%), followed by interns (8, 23.5%) and attending physicians (7, 20.6%). Only one case involving a nurse was identified in Period 2 (2.9%). Other behavior-related issue included communication gaps (18, 26.9% in Period 1 vs. 8, 18.6% in Period 2) and inappropriate family behavior (2, 3.0% in Period 1 vs. 1, 2.3% in Period 2).
DISCUSSION
This is the first study to determine the incidence of ethical issues identified by ICU nurses in their everyday clinical practice and to assess the changes in ethical issues over a decade in a Korean tertiary referral hospital. The data show a reduction in the overall incidence of reported cases involving ethical issues, decreasing from 2.1% (89 cases) of overall admissions to 0.5% (51 cases) over a 10-yr period. Behavior-related issues were the most important issues encountered by ICU nurses. Inappropriate healthcare professional behavior mainly involving resident physicians predominated over the past decade.
To date, few investigations to estimate the frequency of ethical issues or conflicts have been reported. Some ICU caregivers believe that conflicts are frequently identified (6, 8). A recent large cross-sectional survey showed nearly 70% of all ICU caregivers experienced conflicts within last week in ICUs (6). Studdert et al. (8) reported that conflicts occurred for nearly one-third of patients with prolonged ICU stays during their hospitalization. However, conflict incidence seems to be low in other studies that have investigated the effect of ethical intervention for ICU patients (20, 21). In a study on adult ICUs of seven US hospitals during 26 months, 551 cases were involved in ethical conflicts (21). In a study of Asian country, Chen et al. (20) identified only 65 cases involving ethics consultation in a large hospital over 30 months. We also observed a relatively low incidence of cases with ethical issues from the point of ICU nurses.
The main finding in this study was a significant reduction between the incidence of cases with ethical issues recognized by ICU nurses in Period 1 and 2. As hypothesized, the decrease in ethical issues related to LST from the nursing perspective seemed to have contributed to the decreased incidence in this hospital during Period 2. Fassier et al. (22) suggested caregivers' attitudes toward EOL decision played a significant role to resolve the ethical conflicts involved in EOL care. Consensus guidelines for withholding/withdrawal of LST, published by the Korean Medical Association, Korean Academy of Medical Science, and Korean Hospital Association were disseminated among physicians in October 2009 (15). The studied hospital ethics committee has adopted and educated physicians about these guidelines to improve physician's attitude and performance of EOL cares (14). The improvement of organizational factors including the full-time intensivists and the number of nurses has been recommended for optimal EOL care practice (23). Along this line, the enhanced staffing in the studied ICUs (Table 2), might be another contributing reason in part to the decrease in the incidence of ethical issues about LST. The improvement in ICU staffing can alleviate job strain in ICUs. Improved work-related factors, including workplace climate and workload, could positively affect nurses' moral distress and ethical work environment (24), which may ameliorate the occurrence of ethical issues identified by ICU nurses in the studied ICU.
A consistent finding is that the principal cause of ethical issues, from nurses' points of view in both Periods, was related to healthcare professional behavior. In accordance with our results, a recent large, cross-sectional survey reported that approximately half of ICU conflicts originated from behavior-related issues (6). Healthcare professional's behavior-related issues have been more frequently considered as quality improvement or risk management issues rather than as ethical issues. In fact, previous research regarding the resolution of ethical issues or conflicts has focused on EOL care-related issues (7, 8, 25), and even in clinical studies of ethics consultation (26, 27). In several qualitative case studies, however, behavior-related issues, such as lack of communication within ICU teams and inappropriate ICU caregiver behavior, have been described on ethical issues in the ICU (17, 18, 19). Behavior-related issues frequently could contain ethical problems deteriorating involved healthcare professionals' job performances in ICUs, and demand immediate resolution of the conflicts to relieve unnecessary emotional burden between ICU caregivers. In this study, behavior-related issues predominantly involved resident physicians. Resident physicians work long hours in a stressful environment and spend most of their time in the ICU taking care of acutely ill patients. Young intensivists, including interns and resident physicians have experienced higher levels of burnout (6, 28). This, in turn, might be associated with ICU resident physicians' behavior-related issues. Many resident physicians recognize the lack of an ethics education program and desire more hands-on training to help resolve ethical issues, such as EOL decision making (29, 30). Thus, systemic approaches are needed to prevent or decrease behavior-related issues of resident physicians, including providing stress management workshops to reduce work-related stress (31), reducing the working hours (32), as well as ethics and communication skills education (33).
Our study had several limitations. First, ethical issues were not easily defined and using a self-reported questionnaire survey might have led to reporting error. Although our study was performed in a prospective fashion on a daily basis to maximize the recall of nurses, the study could still have been influenced by the willingness and capacity of the participants to detect ethical issues. The fast-paced acute care environment could reduce the frequency with which ethical issues were reported. Cultural differences in reporting a colleague's misbehavior may also influence how nurses perceived and reported ethical issues. Second, we used different methods of collecting the self-reported questionnaires by a research nurse in Period 1 and by an intensivist in Period 2. This difference might influence on the study results. Third, we did not have any information regarding the nurses who participated in the study including age, length of time working in the ICUs and personal history, which could affect the nurses' perception of conflicts (5, 6). Fourth, the study was performed in a single tertiary hospital in Korea, and as such, generalization of our results to ICUs with different institutional cultures and resource availability may not be possible.
Nonetheless, this questionnaire survey is the first study that provides the nature of ethical issues and their incidence in everyday clinical practice encountered by ICU nurses. Additionally, no published study has monitored the changes in ICU nurses' perceptions of ethical issues between two one-year periods separated by 10 yr. With these observations, improvement of the ICU environment might have a positive effect on the reduction in the overall incidence of ethical issues. Moreover, this study suggests behavior-related issues may have a significant contribution to ethical issues from the nursing perspective. Among them, inappropriate healthcare professional behavior predominated, and primarily involved resident physicians. Further study is needed to enhance the ethical environment in the ICUs with systemic approaches to solve behavior-related issues of resident physicians. The results of this study may help to improve the ethical environment in similar ICU settings.


 XML Download
XML Download