

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cerebral palsy (CP) is defined as a group of permanent disorders characterized by impaired movement and posture caused by nonprogressive damage in the motor control centers of the developing fetal or infant brain (1). The clinical picture of CP ranges from mild monoplegia with normal intellect to severe total body spasticity and intellectual impairment (2). In addition, CP can be associated with comorbidities such as epilepsy, gastrointestinal problems, bladder control problems, ocular abnormality, and pain (3, 4). Therefore, a multidisciplinary approach should be used to effectively manage patients with CP.
Muscle and joint contracture and bony deformity frequently occur in patients with CP, especially the spastic type, and therefore orthopedic interventions are often required. The two major surgical procedures used are single event multilevel surgery (SEMLS) for gait improvement and hip reconstructive surgery for pain reduction and facilitation of caregiving. SEMLS has become standard treatment to improve gait in ambulatory patients who are at Gross Motor Function Classification System (5) (GMFCS) level I to III (6). Hip reconstructive surgery is usually performed for patients at GMFCS levels IV and V who have hip instability (7, 8).
The overall medical health of patients with CP is often poorer than that of patients without CP, making them more vulnerable to perioperative complications. Physicians are more focused on postoperative complications related to the procedures or treatment (9, 10, 11), whereas they might be less concerned about intraoperative complications (12). Because complications are more common in patients with CP, surgeons must be aware of perioperative morbidity and prepared to recognize and treat perioperative complications. The purpose of this study was to determine the incidence of perioperative complications associated with lower extremity orthopedic intervention in patients with CP and establish the risk factors for those complications.
MATERIALS AND METHODS
We reviewed the medical records of consecutive patients with CP who were admitted to our hospital and underwent SEMLS and/or hip reconstruction surgery between May 2003 and December 2012. For statistical independence, only data from each patient's first surgery were included in the study (13). Surgery performed under local or regional anesthesia was excluded. Information obtained from medical records included patient age, sex, length of hospital stay, past medical history, involvement of CP, operation time, and surgery details.
SEMLS addresses the correction of all fixed musculoskeletal pathology in one surgical session to improve both gait and gross motor function. The procedures involve tendon lengthening, tendon transfer, rotational osteotomy, and joint stabilization (14). Hip reconstructive surgery involves reduction of the hip joint and correction of bony abnormalities in the femur and acetabulum and soft tissue abnormalities around the hip joint such as adductor release and psoas lengthening (15).
Intraoperative complications
We defined an intraoperative complication as any adverse event occurring in the operating room. Evaluation for Cormack-Lehane (CL) classification (16) and the American Society of Anesthesiologists physical status classification system (ASA class) (17) was performed before initiation of anesthesia to determine if a correlation between the classification system and patient functional level exists. The CL classification is a grading system commonly used to describe the laryngeal view during direct laryngoscopy (18). In grade 1 most of the glottis can be visualized, and in grade 4 neither the glottis nor the epiglottis is visible, making tracheal intubation difficult. ASA class is commonly used to describe preoperative physical status and predict perioperative anesthesia risk (19). There are five classes ranging from completely healthy to moribund and terminally ill (17). To determine if emergence from anesthesia was delayed, the emergence time was calculated as the time between discontinuance of administration of anesthetics and departure time from operation room to postoperative care unit. Studies have reported a relationship between perioperative complications and intraoperative hypothermia (20, 21). Intraoperative hypothermia was defined as core body temperature measured by esophageal stethoscope below 35℃. Hypotension and bradycardia were divided into relative and absolute with relative defined as a 20% decrease from baseline while receiving anesthesia (22). The baseline was the blood pressure and heart rate at midnight the day of surgery. Absolute hypotension and bradycardia were determined by the patients' age group (Table 1) (23).
Postoperative complications
Immediate postoperative complications that occurred during hospital stay were assessed. Complications were divided into major and minor. Major complications were those that resulted in a prolonged hospital stay of more than 5 days or unplanned admission to the intensive care unit (11). Six orthopedic surgeons with 28, 12, 9, 8, and 5 yr of experience and two anesthesiologists with 25 and 6 yr of experience held consensus building sessions before assessing postoperative complications.
Statistical analysis
Patients were stratified into two groups according to GMFCS level: ambulatory (GMFCS I to III) and non-ambulatory (GMFCS level IV and V). They were also divided into three age groups (<13, 13-18, and ≥18 yr) to determine patient distribution and define absolute hypotension and bradycardia. The chi-square test or Fisher's exact test was used to compare categorical variables. The Cochran-Mantel-Haenszel (CMH) test was used to determine relationships between two categorical variables controlling for one or more categorical factors. An independent t-test was used to evaluate the significance of differences in anesthesia emergence time and GMFCS levels. Analysis of covariance (ANCOVA) was used to assess the relationship between operation time and complications, controlling for GMFCS level and hip surgery. Statistical analysis was performed using SPSS version 20.0 (IBM Co., Chicago, IL, USA). All statistics were two-tailed, and P values <0.05 were considered statistically significant.
RESULTS
Initially, 871 patients met our inclusion criteria. Three were excluded because their first surgeries were performed under regional anesthesia, leaving a total of 868 surgeries in 868 patients in the study. The mean age of the patients at time of first surgery was 11.8±7.6 yr (range, 4.0 to 61.0 yr). The mean hospital stay was 10.5±5.9 days (range, 0 to 60 days). Two hundred thirty-five patients underwent proximal femoral osteotomy, and 34 patients underwent pelvic osteotomy simultaneously. Diplegia (54.3%) was most commonly found in involvement of CP, and the most common GMFCS level was II (Table 2). Twenty patients (2.3%) had a history of pneumonia, and four patients (0.5%) had upper airway hypotonia. The majority of the patients were categorized as I and II in CL grade and ASA class (Fig. 1). Twenty (2.3%) patients suffered major postoperative complications, and 35 (4.0%) suffered minor complications postoperatively (Table 3).
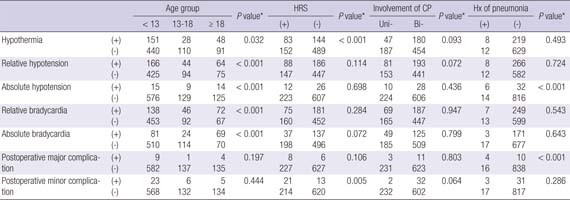
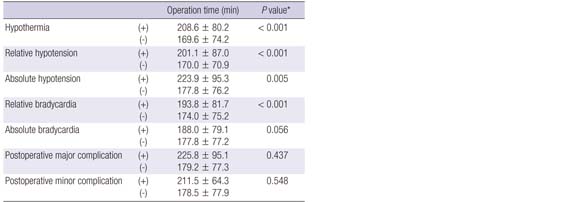
The patients at GMFCS level IV and V had a significantly higher perioperative complication rate compared with those at GMFCS level I to III (Table 4). Because GMFCS level showed a significant association with age group (P=0.003), hip reconstructive surgery, involvement of CP, and history of pneumonia (P<0.001) (Appendix I), the relationships between perioperative complications and these factors were analyzed using the CMH test, adjusting for GMFCS level as a control variable. There was no statistical difference in emergence time from anesthesia according to GMFCS level of the patients (P=0.331). Older age group (P=0.032), lower functional level (GMFCS level IV and V), and hip reconstructive surgery were risk factors for hypothermia during the surgery (P<0.001). Lower functional level, older age, and history of pneumonia were associated with absolute hypotension during surgery (P<0.001). Older age increased the risk of relative and absolute bradycardia during surgery, and lower functional level and history of pneumonia increased the risk of major postoperative complications (P<0.001) (Table 4, Appendix II). After adjustment for GMFCS level and hip surgery, the operation time was longer in patients with hypothermia, relative and absolute hypotension, and relative bradycardia than in patients without these complications (Table 4, Appendix III). There was no relationship between GMFCS level and CL classification, whereas ASA class demonstrated a statistically significant relationship with GMFCS level (P<0.001).
DISCUSSION
Patients with CP have overall poor health than patients without a chronic illness, and they have a higher risk of perioperative complications from anesthesia or the surgical procedure. Since most surgeons have focused on postoperative complications, we performed this study to ascertain the incidence of intra- and postoperative complications in patients with CP and to determine the risk factors for complications associated with surgery. In the present study, GMFCS level, patient age, hip reconstructive surgery, and operation time affected core body temperature during surgery. In addition, major postoperative complications occurred more frequently in patients with lower functional level and history of pneumonia.
In this study, GMFCS level showed a significant relationship with age group, hip reconstructive surgery, involvement of CP, and history of pneumonia. We believed that patients at GMFCS level IV and V required hip reconstructive surgery more frequently during childhood and adolescence. Their medical conditions were usually more severe compared with those of patients at GMFCS level I to III. Therefore, we used the CMH test to analyze the relationships between predisposing factors and perioperative complications adjusting for GMFCS level as a control variable.
Older age group, lower functional level, hip reconstructive surgery, and operation time increased the rate of hypothermia during surgery in this study. The risk of hypothermia tends to be underestimated during surgical procedures. However, hypothermia can delay wound healing and predispose patients to wound infection (20). It can result in peripheral vasoconstriction and neutrophil dysfunction (24), which have been shown to increase the incidence of surgical wound infections by a magnitude of three, and substantially reduced the immune system response to infection (25). Furthermore, hypothermia during surgery adversely affects the coagulation system through impaired platelet function and prolonged prothrombin and clotting time (25). Maintaining body temperature during surgery can decrease the incidence of postoperative wound infection and delayed wound healing.
Lower functional level, older age, history of pneumonia, and operation time were associated with absolute hypotension during surgery. Relative and absolute hypotension were observed in 31.6% and 4.4% of the study population, respectively, which is consistent with previous studies (26, 12). The cause of hypotension was multifactorial and may have been associated with an increased sensitivity to anesthetic drugs or decreased central adrenergic activity related to CP. Although intraoperative hypotension may be associated with a higher postoperative morbidity (27), its clinical significance has not yet been established. Understanding, early recognition and management of hypotension is important in patients with CP, who have less physiological reserve and insufficient compensatory responses to maintain normal blood pressure.
In the last decade, 868 patients with CP underwent surgery at our hospital. Cardiac arrest occurred in three patients in the early postoperative period. All occurred on the ward, and cardiopulmonary resuscitation was initiated immediately with return of spontaneous circulation within 5 to 17 min. The age of the patients varied (9, 16, and 20 yr old), as did the cause of cardiac arrest (seizure, aspiration pneumonia, and laryngospasm); however, all three patients were GMFCS level V. These patients represent 5.5% (3/55) of all study subjects at GMFCS level V. A previous study showed that ambulatory function in patients with CP was highly correlated with the risk of complications, including life-threatening events, after orthopedic surgery (28). Two patients in the study were ASA class 3, and one patient, who arrested immediately after laryngeal suction, was ASA class 2 and had suffered from a recent upper respiratory infection. Patients with CP often have an impaired ability to clear pharyngeal secretions, resulting in the pooling of secretions in the oropharynx (12). Furthermore, CP patients, including those at GMFCS level I and II, have a reduced aerobic capacity compared to patients without CP (29). A previous study reported that spasticity in CP patients can cause local obstruction of venous return in leg muscle, leading to a reduced cardiac output and oxygen delivery (30). This phenomenon may, in part, explain the reduced peak oxygen uptake seen in patients with CP (29). Studies show that, even prior to surgery, most CP patients and their parents focus on improving physical function rather than general overall medical condition including respiratory problems (31). This tendency leaves patients far more vulnerable to perioperative respiratory complications, especially in patients at a lower functional level. Respiratory complications are one of the life-threatening conditions for CP patients undergoing orthopedic intervention, therefore the importance of preservation and early recovery of perioperative respiratory function should be emphasized.
ASA class showed a positive relationship with patients' GMFCS level. ASA class is a readily available patient assessment tool used prior to the administration of anesthesia. Although no grading system can predict specific clinical complications, ASA class reflects a patient's general medical condition and can provide useful information to estimate the risk of postoperative morbidity (32, 33). Physicians should pay careful attention to ASA class, because it can help to avoid adverse postoperative outcomes, especially in patients at a lower functional level such as GMFCS level IV and V. An intra- and postoperative multidisciplinary approach encompassing the respiratory, cardiovascular, gastrointestinal, neurological, and urological systems would help improve evaluation of the overall risks other than surgical treatment prognosis and aid in optimizing medical treatment.
There is a limitation in our study. Because the study design was retrospective, the accuracy of the incidence calculation was dependent upon the completeness of the medical records from which the data were obtained.
This study was performed to determine the incidence of intraoperative and postoperative complications in patients with CP and establish the risk factors for these complications. Our results suggest that GMFCS level, patient age, hip reconstructive surgery, history of pneumonia, and operation time are associated with adverse effects on intraoperative body temperature, the cardiovascular system, and immediate postoperative complications. Recognition of risk factors for complications and careful pre- and postoperative multidisciplinary approach can help CP patients in their optimal medical condition during the perioperative period.



 XML Download
XML Download