

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since statins have a preventive role in primary and secondary prevention of coronary artery disease (1, 2, 3), several prospective trials have been conducted to identify the favorable effects of statin before percutaneous coronary intervention (PCI) (4, 5, 6, 7). In those trials, atorvastatin pretreatment in patients undergoing PCI for stable angina and non-ST-segment elevation myocardial infarction reduced myocardial damage and improved clinical outcomes. However, it is uncertain whether pretreatment of high dose of statins in patients with ST-segment elevation myocardial infarction (STEMI) can reduce infarct size. To answer this question, we conducted a prospective randomized trial to evaluate the effects of atorvastatin pretreatment on infarct size in patients with STEMI (AT-STEMI) (8). In this study, pretreatment with high-dose atorvastatin followed by further treatment for 5 days did not reduce infarct size measured by single-photon emission computed tomography (SPECT). Although infarct size measured by SPECT has been reported to be a surrogate for clinical outcomes (9), contrast enhanced magnetic resonance imaging (CE-MRI) is superior to myocardial SPECT in measuring infarct size, especially when the infarct burden is small and nontransmural (10, 11, 12). In addition, CE-MRI can assess the area at risk (AAR), microvascular obstruction (MVO), and myocardial hemorrhage in patients with myocardial infarction (13, 14, 15). Therefore, we used CE-MRI to evaluate the efficacy of atorvastatin pretreatment in patients undergoing primary PCI for STEMI. This study is a prespecified substudy of the AT-STEMI trial.
MATERIALS AND METHODS
Study design and patients
The AT-STEMI trial was a prospective randomized, multicenter study designated to evaluate the impact of high-dose atorvastatin pretreatment on myocardial infarct size in patients undergoing primary PCI for STEMI (8). This trial was registered with ClinicalTrials.gov, NCT00610870. Patients from 5 major coronary intervention centers in Korea were enrolled between August 2007 and February 2009. Patients were eligible if they had STEMI less than 12 hr after symptom onset. STEMI was defined as ST-segment elevation of at least 1 mm in two or more continuous leads on the electrocardiogram (ECG). Exclusion criteria were cardiogenic shock, previous MI, chronic liver disease, and current statin use. We planned several substudies including using MRI before initiation of the AT-STEMI trial. All patients enrolled at the Samsung Medical Center, one of the participating centers, were candidates for the MRI substudy.
Study protocol and procedure
The study protocol was described previously (8). Briefly, patients were randomly assigned to the atorvastatin group or the conventional primary PCI (control) group. Randomization was stratified by the hospitals and the location of infarction. In the atorvastatin group, 80 mg of atorvastatin was administrated as early as possible after randomization. All patients received 300 mg aspirin and 600 mg clopidogrel before PCI if they had not previously taken these medications. Intravenous heparin was administered to maintain an activated clotting time of 300 sec. Glycoprotein IIb/IIIa receptor antagonist was used at the operator's discretion. Coronary angiography and stent implantation were performed using standard interventional techniques. After the procedure, 80 mg atorvastatin was maintained for 5 days, and then the dose of atorvastatin was decreased to 10 mg/day for the atorvastatin group. In the control group, treatment of 10 mg atorvastatin was initiated the day after primary PCI. Thereafter, atorvastatin was titrated to reduce low-density lipoprotein cholesterol <1.8 mM/L (70 mg/dL) in both groups. The myocardial band fraction of creatinine kinase (CK-MB) was measured before PCI, and every 8 hr for 2 days after the procedure. After 2 days, CK-MB was measured once daily until the level of enzyme was normalized. Twelve-lead ECGs were obtained before and at 60 min after the procedure (8).
Data analysis
Baseline characteristics, angiographic and procedural data, medication use, and outcome data were recorded and collected by dedicated research coordinators. ECG and angiographic data were analyzed independently at the angiographic core laboratory of the Samsung Medical Center (Seoul, Korea). The total ST-segment elevation was measured manually from leads exploring infarct area (16). Complete ST-segment resolution was defined as a decrease >70% in ST-segment elevation by comparing before and 60 min after PCI. Evaluation of myocardial blush grade (MBG) was performed using the angiograms made at the end of the index procedures as previously described: 0= absence of contrast opacification in the myocardial infarct zone or persistent staining without washout, 1=minimal contrast opacification, 2=reduced but clearly evident blush in the infarct zone compared to the ipsilateral or contralateral noninvolved epicardial vessels, and 3=myocardial contrast filling equal to or greater than that seen in the noninvolved epicardial vessels (17).
CE-MRI protocol and analysis
Between days 5 and 14, CE-MRI consisting of cine, T2 weighted imaging, first pass perfusion and delayed enhancement imaging was performed. A 1.5 Tesla magnetic scanner (Achieva, Philips Medical Systems, Best, the Netherlands) was used (19, 20). Cine MRI images were obtained using a fast gradient echo sequence after scout and localizer image acquisition. Slice thickness was set at 6 mm and short-axis images of the left ventricle (LV) were acquired from the apex to base. Temporal resolution was 25-30 frames per RR interval. T2-weighted MRI was performed in the cardiac short-axis using an inversion recovery fast-spin echo sequence. For the first pass images of contrast, a dose of 0.15 M/kg gadolinium-diethylenetriamine pentaacetic acid (Magnevist, Bayer Schering Pharma, Berlin, Germany) was injected intravenously followed by a saline flush. T1-weighted dynamic sequence was performed with 6 mm slice thickness, 40×40 cm field-of-view and 128×128 image matrix. Delayed enhancement and microvascular obstruction (MVO) were evaluated 15 min after the administration of gadolinium in 10-12 continuous slices of 6 mm thickness with a 4 mm interslice gap using a multi-shot turbo field echo breath-hold sequence with nonselective inversion. The inversion delay time was varied in the range of 200-300 ms using a Look-Locker system.
Image analysis was performed using commercial analysis software, Cardiovascular Angiographic Analysis System (CAAS MRV version 1.0, Pie Medical Imaging B.V., the Netherlands) (19, 20). Left ventricular volume and ejection fraction were measured by contouring the endocardial and epicardial border of myocardium in the short-axis images acquired at the end diastole and systole. Myocardial mass was calculated by multiplying the myocardial volume by myocardial density (1.05 g/mL). The infarct volume was quantified by manual drawing of the delayed hyperenhanced lesion within each segment of the short-axis images, multiplied by the slice thickness to include the entire LV. The volume of perfusion defect and MVO were calculated in same manner. The presence of myocardial hemorrhage, defined as a central core of hypointense signal within an area of increased T2 signal intensity, and myocardial AAR, defined as a myocardium with signal intensity greater than 2 SDs above the mean signal intensity of remote normal myocardium, were quantified in a T2-weighted image using a similar algorithm. Additionally, the myocardial salvage index was computed as follows: myocardial salvage index=(AAR-infarct size)×100/AAR (18). The infarct transmurality for each segment was calculated by dividing hyperenhanced area by the total area of affected myocardium. The transmural infarction was defined as the segments with >75% of infarct transmurality (19, 20).
Study end points
The primary end point was myocardial infarct size as assessed by CE-MRI. The secondary end points included myocardial salvage index and MVO area assessed by CE-MRI. MBG, complete ST resolution, and peak CK-MB level after the procedure were also compared between the atorvastatin group and control group.
Statistical analysis
The expected standard deviation of myocardial infarct size was estimated to be 10% based on the previous study (21), and a difference >7.5% would be regarded as significant. For a power of 0.80 and an α error of 0.05, the estimated sample size needed would be 29 patients in each group (8, 19, 20).
All analyses were performed with SPSS software version 17.0 (SPSS Inc, Chicago, IL, USA). Continuous variables were analyzed using Student's t-test or the Wilcoxon rank-sum test where applicable. Categorical data were tested using Fisher's exact test or the chi-square test. The threshold for statistical significance was chosen as P=0.05 in the 2-tailed tests.
RESULTS
Baseline characteristics and procedural data
From August 2007 to February 2009, a total of 218 patients were enrolled in the AT-STEMI trial, and 87 patients enrolled in the Samsung Medical Center were candidates for the MRI substudy. Of these, CE-MRI was not performed due to claustrophobia (n= 2) or metallic implant within the body (n=1). Furthermore, 15 patients did not undergo CE-MRI because of hemodynamic instability after the enrollment (n=6), or patient refusal (n=9). After excluding inadequate MRI images from analysis (n=2), CE-MRI data were ultimately available for 30 patients in the atorvastatin group and 37 patients in the control group. Overall subject characteristics including clinical presentations and initial laboratory findings are presented in Table 1. There was no significant difference in baseline clinical and laboratory characteristics between the two groups.
Table 2 shows the angiographic and procedural findings of the two groups. The atorvastatin group tended to have a lower grade of TIMI flow than the control group, but this difference was not statistically significant. Most patients of the two groups underwent implantation of stents in the culprit coronary arteries. Drug-eluting stents were used predominantly, with no difference between the study groups. The stent diameter and length were similar in the two groups. There were no significant differences in medication during hospitalization and follow-up period (Table 3).
Angiographic, ECG, biochemical, and clinical outcomes
No angiographic reflow, final TIMI flow grade, and final MBG did not differ between the atorvastatin and the control group (P=0.45 for no reflow, P=0.09 for final TIMI flow grade, and P=0.43 for final MBG) (Table 4). Similarly, both groups had comparable incidences of complete ST-segment resolution at 60 min (60% vs. 56.8%, P=0.79). No significant difference was found in the level of peak CK-MB between the 2 groups (226.3±140.9 vs. 174.1±147.3, P=0.15).
Complete clinical follow-up data were obtained for all patients. The 6-month major cardiac event rate was not significantly different between the atorvastatin group and control group.
CE-MRI findings
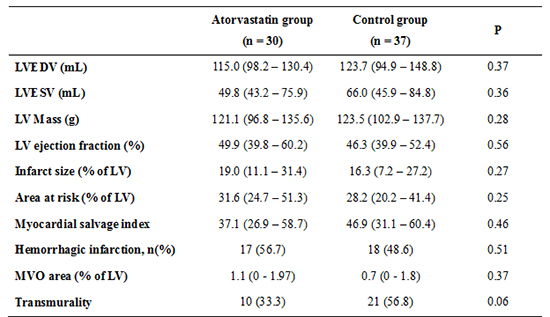
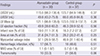
There was no difference in the intervals from procedure to MRI between the groups (9.5 [6-18.3] vs. 8 [5-12.5], P=0.17). Table 5 shows data analyzed from the cine, T2-weighted and CE-MRI of the atorvastatin and control group. The LV end diastolic volume, end systolic volume, and ejection fraction measured by MRI were similar in both groups. The primary end point, infarct size on CE-MRI after the atorvastatin pretreatment and procedure was not significantly different between the two groups (19% [11.1-31.4] vs. 16.3% [7.2-27.2], P=0.27). Additionally, the myocardial salvage index (37.1% [26.9-58.7] vs. 46.9% [39.9-52.4], P=0.46) and the extent of MVO (1.1% [0-1.97] vs. 0.7% [0-1.8], P=0.37) were not lower in the atorvastatin group compared to the control group. There were no significant differences of the incidence of hemorrhagic (56.7% vs. 48.6%, P=0.51) or transmural infarctions in both groups (33.3% vs. 56.8%, P=0.06).
DISCUSSION
In this randomized study, we compared CE-MRI recordings to evaluate the efficacy of high dose atorvastatin loading followed by further medication for 5 days after PCI on the extent of myocardial infarction in patients undergoing primary PCI for STEMI. Our data indicate that infarction severity does not change after atorvastatin pretreatment in STEMI patients. There was no significant difference in the infarct size, AAR, MVO area, infarct transmurality, a frequency of hemorrhagic infarction, or the proportion of myocardial salvage between the atorvastatin group and controls. Moreover, post-procedural TIMI flow grade, MBG, complete ST-segment resolution at 60 min, and the peak CK-MB level was similar in both groups.
The AT-STEMI and STATIN STEMI trials report that high-dose atorvastatin pretreatment before PCI did not show significant improvement of clinical outcome (8, 22). However, these 2 trials have too few numbers of participants to draw conclusions regarding the clinical outcome including major adverse cardiac events. Although infarct size measured by SPECT was primary end point in the AT-STEMI trial, SPECT has low sensitivity in cases of small myocardial infarctions or non-transmural infarctions. Furthermore, the STATIN STEMI study showed that secondary end points such as MBG and complete ST segment resolution were improved in the atorvastatin group. In the AT-STEMI trial, the high-dose atorvastatin pretreatment group demonstrated absolutely 5.2% reduced incidence of major adverse cardiac events at 6 months (8). Considering these doubtful conclusions, larger randomized trials or more obvious surrogate parameters as primary end points are required to confirm the effects of atorvastatin pretreatment. Therefore, our study may have strengths with respect to performing a planned substudy using CE-MRI-derived infarct size as the primary end point. In addition, CE-MRI is a reliable tool to detect morphologic and functional sequelae of myocardial infarction and provide a broad range of pathophysiological information such as the presence of scars, edema, and the viability of myocardium. CE-MRI might demonstrate more concrete impacts of atorvastatin pretreatment on injured myocardium that are not detected by other diagnostic modalities.
Although statins are known to have anti-inflammatory, antithrombotic effects and also known to improve endothelial function and myocardial circulation (24, 25), atorvastatin pretreatment did not reduce infarct size measured by CE-MRI in the present study. Moreover, the myocardial salvage index, which is an attractive CE-MRI parameter from a pathophysiological point of view, was not different between the atorvastatin and control group. MVO and hemorrhagic infarction, which are known to be predictors of adverse LV remodeling, as well as the risk of cardiovascular events did not show any differences between the 2 groups (26, 27). Our findings were supported by another CE-MRI study. In the REPERATOR trial, Post et al. reported that pretreatment with atorvastatin in an acute myocardial infarction does not result in an improved cardiac function, microvascular perfusion, or decreased myocardial infarct size (23). Although the comprehensive analysis of CE-CMR such as MVO and hemorrhagic infarction and a slightly larger number of enrolled patients are advantages of our study over the REPERATOR trial, they elegantly performed serial CE-MRI studies within 1 day, at 1 week, and 3 months follow up. Based on the results of both studies, it seems unlikely that high dose atorvastatin pretreatment in patients undergoing PCI for STEMI can reduce injury of myocardium.
This ineffectiveness of atorvastatin pretreatment in STEMI patients might be explained by severe ischemic burden or injury which cannot be prevented or reduced by a single dose of atorvastatin before primary PCI. The interval between atorvastatin administration and reperfusion might be too short for atorvastatin to initiate its action since the median door-to-balloon time was 81 min in the atorvastatin group (8, 20).
Our study has several limitations. First, the sample size is not large, although calculations were conducted by standard methods based upon preliminary data. Second, only patients suitable for MRI examination were included. Therefore, the number of enrolled patients in each group was different. Unstable patients with hemodynamic compromise or severe arrhythmia were excluded from the study, which may have caused selection bias. Third, the timing of CE-MRI was widely distributed. However, CE-MRI was done within 14 days after primary PCI in all patients and there was no significant difference in interval from the index procedure to obtaining MRI between the 2 groups. Moreover, we did not undergo follow up CE-MRI, which might be more closely related to final myocardial damage. Fourth, this was not a placebo-controlled study. However, the primary end point was assessed independently and blindly at the core laboratory, and therefore we believe that this study design has little effect on the results. Lastly, our study has broad inclusion criteria. Because of the small sample size, we could not perform the subgroup analysis on patients who have a short time from symptom onset to ballooning or who are present with anterior wall infarction, which might have a better outcome in the atorvastatin pretreatment group.
To conclude, in this CE-MRI substudy of AT-STEMI trial, a high dose atorvastatin pretreatment followed by 5 days of further treatment did not reduce the infarct size in in patients undergoing primary PCI for STEMI. The present study suggests that atorvastatin preloading does not improve clinical outcomes in patients with STEMI.

 XML Download
XML Download