

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Pyrethroids are widely used for agricultural, and house hold purposes due to their high insecticidal activity, environmental stability, and relatively low acute mammalian toxicity (1, 2). Pyrethroids are classified into type I and type II based on the chemical structure and intoxication syndromes following intravenous or intracerebral administration to rodents (1). Since type II pyrethroids are more potent insecticides, type II pyrethroid poisoning is more common than type I pyrethroid poisoning (3). Type II pyrethroids accounted for more than 99.9% of cases of pyrethroid poisoning in China (4). However, despite extensive worldwide use, and high accountability for insecticide poisoning, there are only a few studies reporting the clinical features of acute type II pyrethroid poisoning in humans (5). Also, no report on the factors that can be used during the early stage of type II pyrethroid poisoning to assess the patient outcome has been published.
The association of hyperglycemia with mortality has been reported in methanol or aluminum phosphide poisoning as well as in acute diseases such as acute myocardial infarction, ischemic stroke, and trauma (6, 7, 8). Hyperglycemia has an adverse effect on the outcome of acute disease through several mechanisms including increased oxidative stress, impairment of leukocyte function, induction of apoptosis of cells, intra- and extracellular dehydration, and stimulation of inflammation (9, 10). However, such an association has not been demonstrated in pyrethroid poisoning. Because blood glucose levels can be easily measured anywhere, and hence, evaluation of the prognostic value of hyperglycemia in type II pyrethroid poisoning is clinically valuable for physicians who treat patients with type II pyrethroid poisoning at an early stage and determine the patients' disposition.
The purpose of this study was to review the clinical and laboratory features of type II pyrethroid poisoning, and to determine whether hyperglycemia at presentation is a prognostic factor in type II pyrethroid poisoned patients.
MATERIALS AND METHODS
Study design and setting
This was a single institutional retrospective cohort study performed by chart review. This study was conducted at Chonnam National University Hospital, a tertiary care teaching facility comprising an emergency department (ED) that provides care for approximately 45,000 patients per year.
Patients
The inclusion criteria consisted of 18 yr of age or older who presented to our ED after pyrethroid ingestion between 2003 and 2014 and underwent the glucose testing at presentation. The diagnosis of pyrethroid ingestion was made based on the history of pyrethroid ingestion that was provided by the patients or the witness, and the respective hospital records with the physician's notation of "pyrethroid" after he had checked the bottle brought by the patients or the witness. Through this review, 132 patients were identified.
The exclusion criteria consisted of mixed ingestion, including ethanol, type I pyrethroid ingestion and a history of renal failure. We excluded patients who had a history of co-ingestion of pyrethroid with ethanol because ethanol can influence glucose levels (11). Additionally, patients who were given fluids containing glucose before the measurement of glucose levels at presentation were excluded. Thus, data from a total of 104 patients were included in the analysis.
Data collection and analysis
The medical records were reviewed by an assistant, who was unaware of the purpose of the study, and the following data were collected: age, gender, comorbidity, chemical compound and the amount of type II pyrethroid ingested, history of administration of gastric lavage or activated charcoal, the time interval from ingestion to arrival at our ED, initial vital signs, electrocardiographic (ECG) findings, blood glucose level at presentation, results of laboratory tests, complications, length of hospitalization, and the cause of death. The amount of type II pyrethroid ingested was estimated as a spoonful (5 mL), a mouthful (25 mL), a cup (100 mL), and a bottle (300 mL) (12). The initial blood glucose level at presentation was obtained by performing a routine blood test. Hyperglycemia was defined as a glucose concentration >200 mg/dL (13). ECGs were interpreted by an emergency physician who was blinded to the patients' clinical data. The corrected QT interval (QTc) was calculated using the Bazett's formula (QT divided by the square root of RR). The prolongation of a QTc interval was defined as a QTc interval greater than 440 ms. Medical complications included the following: acute kidney injury, respiratory failure, hypotension (the need for pressor support to maintain blood pressure after admission), acidosis (pH<7.20), seizures, cardiac arrest or death. Acute kidney injury was defined as an absolute increase in serum creatinine (Cr) of ≥0.3 mg/dL (26.52 µM/L) or a percentage increase in the serum Cr≥50% from baseline. Respiratory failure was defined as the need for mechanical ventilation. In addition, any other conditions encountered during the review of patient medical records that were deemed to be serious and clinically significant by the investigator were considered as medical complications.
To demonstrate the association between hyperglycemia at presentation and patient outcome, the patients were divided into two groups according to the presence of DM, because the cut off value of blood glucose level differs according to the presence of DM in other acute illness (14). The presence of DM was determined based on a previous clinical or biochemical diagnosis of DM, or treatment with oral hypoglycemic agents or insulin. Also, when the fasting plasma glucose level was higher than 120 mg/dL or the postprandial plasma glucose level was 200 mg/dL at discharge, the patients were considered as having DM. Then the patients were subsequently divided into two groups based on the development of complications. Patients who developed a medical complication during hospitalization were assigned to the complicated group.
The predictive value of hyperglycemia at presentation was determined by univariate analysis. Also, for identifying other predictive factors associated with a high risk for complications, objective variables that could be easily assessed at presentation or that were previously reported as predictor variables such as age, intentional ingestion, Glasgow coma scale (GCS), radiologic findings, and WBC were also evaluated (15). However, variables such as the result of arterial blood gas analysis, and systolic blood pressure were excluded because they were used to define complications such as hypotension and acidosis, and also because the patients who had these conditions at presentation were assigned to the complicated group. Univariate analysis of the association between the covariates and the outcome was performed. Covariates with P values less than 0.05 were considered sufficient for the inclusion of a variable in the multivariate logistic regression analysis. Odds ratios (ORs) and confidence interval (CI) were calculated for all significant variables. All statistical analyses were performed using the Statistical Package for the Social Sciences version 21.0.
RESULTS
Patient characteristics
Baseline characteristics and clinical course of the 104 patients who were enrolled in this study are summarized in Table 1. The complication rate and mortality rate was 26.9% and 2.9% in type II pyrethroid poisoned patients. Eleven (10.6%) patients had DM. Diabetic patients had a higher frequency of complications compared to non-diabetics patients (63.6% in diabetics vs. 22.6% in non-diabetics, P value=0.004), but there was no significant difference in mortality between the two groups. (9.1% in diabetics vs. 2.2% in non-diabetics, P value=0.193).
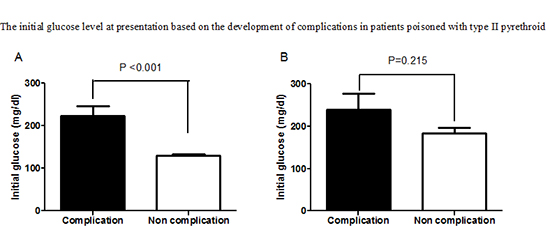
In the 93 non-diabetic patients, complicated patients showed a higher frequency of hyperglycemia, abnormalities on the initial radiograph, depressed mentality (GCS≤13), lower PaCO2, and HCO3- levels, and higher WBC and AST levels at the time of admission than non-complicated group (Fig. 1, Table 1).
In the 11 diabetic patients, complicated group had a higher frequency of depressed mentality and a lower blood urea nitrogen (BUN) level at admission. However, the glucose level at presentation and frequency of hyperglycemia did not differ according to the development of complications (Fig. 1, Table 1).
Outcome
Twenty eight (26.9%) patients experienced at least one complication during hospitalization, and the most common complications were respiratory failure (21.2%) (Table 2). The incidences of acidosis, hypotension, and renal failure were significantly higher in diabetic patients than in non-diabetic patients.
All of the complications developed within 24 hr after presentation. Three patients died because of refractory hypotension and azotemia accompanied by hyperkalemia and metabolic acidosis. Cardiac arrest developed in a 26-yr-old male who had ingested 600 mL of cypermethrin. He underwent a therapeutic hypothermia, and regained an alert mentality with a normal lifestyle at discharge.
Risk stratification
In the 93 non-diabetic patients, hyperglycemia, GCS ≤13, WBC, AST, and X ray abnormality were included in multivariate analysis. The ingested amount variable was not included in the multivariate analysis, even though a significant difference was found for the development of complications in a univariate analysis, because it is possible the reported information is inaccurate. Hyperglycemia at presentation and GCS ≤13 were independent factors for predicting complications in non-diabetic type II pyrethroid poisoned patients. The ORs for hyperglycemia were higher than the ORs for GCS score (Table 3).
However, in 11 diabetic patients, none of the investigated variables showed a significant difference in the development of complications in multivariate analysis probably because of small number of diabetic patients (data not shown).
DISCUSSION
Multiple isoforms of targeted sodium channels with varied sensitivities to pyrethroids, rapid metabolism to nontoxic substances by liver enzymes, cell membrane lipids with lower avidity, and a relatively high body temperature contribute to lower acute toxicity of pyrethroids in mammals (15). However, despite a relatively lower acute toxicity of pyrethroids in mammals, type II pyrethroid poisoning is not a mild disease, and it had mortality rate of 2.9% and a complication rate of 26.9% in this study.
The most common complication found in this study was respiratory failure followed by acidosis and hypotension. Similarly, Cha et al. (15) reported that respiratory failure requiring a mechanical ventilator is the most common symptom of type I or II pyrethroid poisoning. Other complications, such as seizure, cardiac arrest, acute renal failure, arrhythmia, takotsubo cardiomyopathy and death, have been reported for pyrethroid poisoning (15, 16).
Consistent with previous results, gastrointestinal tract symptoms, such as nausea and vomiting, followed by depressed mentality (GCS ≤13) were the most common symptoms reported in our study (15, 16). Solvents, such as xylene and surfactant, were suggested to play a role in the development of gastrointestinal tract symptoms (15).
Consistently with previous study including 59 type I or II pyrethroid poisoned patients, an altered mental status at presentation (GCS ≤13) was an independent factor for complication (15). Modification of sodium, chloride, and calcium channels in the neurons and the effect of pyrethroid on peripheral type benzodiazepine receptors associated with the GABA receptor contribute to the development of the central nervous system symptoms in pyrethroid poisoned mammals (1). Many commercial pyrethroid insecticides contains hydrocarbon as the solvent vehicle. The vehicle also partially contributes to the development of an altered mental state. In a reported case of a patient poisoned with deltamethrin insecticide, altered mental state with apnea and asystole unresponsive to catecholamines were due to the effect of the hydrocarbon that was used as a solvent rather than to deltamethrin action (17).
The mechanism of hyperglycemia in pyrethroid poisoning is not clear. Blood glucose, and plasma noradrenaline and adrenaline levels in rats were increased following treatment with deltamethrin (3, 18). The increased adrenalin level may be one of the mechanisms for the increased blood glucose level. The physiological responses to choreoathetosis induced by pyrethroid neurotoxicity and the action of pyrethroid on the supraspinal centers were proposed as one of the underlying mechanisms (19, 20). The alternative mechanisms for hyperglycemia may be an impairment of insulin secretion from the pancreatic islets due to the effect on voltage sensitive calcium channels and stress induced hyperglycemia. Development of pancreatitis (lipase > 100 U) with mild abdominal pain developed 7 days after ingestion in one patient who experienced acidosis and respiratory failure. Acute pancreatitis in this patient may be suggestive of the effect of type II pyrethroid on the pancreas. Regardless of the mechanism for hyperglycemia, hyperglycemia induces increased oxidative stress, impairment of leukocyte function, induction of apoptosis of cells, intra- and extracellular dehydration, and induction of inflammation (1, 9). This mechanism may account for the association between hyperglycemia and poor outcome in several diseases (6, 7, 8). Also, in our study, hyperglycemia was an independent predictive factor for complications in non-diabetic type II pyrethroid poisoned patients. The patients who have hyperglycemia should be considered at a high risk for developing complications. However, further studies are needed to determine whether controlling hyperglycemia may have a therapeutic benefit.
In diabetic patients, GCS and BUN levels were found to be significant in the univariate analysis, but were not significant in the multivariate analysis. This can be attributed to the small number of diabetic patients. Considering higher incidence of complication in diabetic patients, a further study with a large number of diabetic patients is needed.
This study has several limitations. First, this study was performed in one center and the results may lack wider applicability. Second, the sample size of this study was not sufficient to derive strong conclusions. Especially, the number of non-diabetic patients who experienced complications and the number of patients who had DM were relatively low. A prospective study with a large number of patients is needed to validate these findings. Third, in this study, we only demonstrated the association between the blood glucose level and the outcome. To find answers to the questions such as, what is the cause of an increased blood glucose level, and whether glycemic control has an effect on outcomes; a large, randomized study needs to be performed.
In conclusion, type II pyrethroid poisoning has a complication rate of 26.9% in humans, which is contrast to the relatively low acute toxicity of pyrethroids in other mammals. Hyperglycemia at presentation may be useful to predict the critical complications and to determine a disposition of non-diabetic type II pyrethroid poisoned patients.



 XML Download
XML Download