

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Heart failure is a leading cause of death in developed countries (1). Cardiac resynchronization therapy (CRT) with multisite ventricular pacing was first conceived (2) based on the finding that approximately one third of patients with advanced heart failure (HF) have prolonged ventricular conduction (3). Multiple large-scale clinical trials have shown that CRT modifies ventricular electromechanical delay, induces improvements in ventricular structure and function (4), leads to better exercise tolerance and quality of life (5, 6), and reduces mortality and hospitalization rates (7, 8).
These trial results led to the acceptance of CRT into current clinical practice guidelines (9, 10). However, there are still some controversies on specific indications for CRT in patients with HF. These disagreements mainly stem from questions of who would most and least benefit from CRT (11, 12, 13). The most debated issues include optimal QRS duration and morphology, etiology (ischemic or not), and baseline functional capacity. Recent trials, which sought to expand the indication for CRT, showed variable and conflicting results (14, 15, 16, 17, 18).
Given the broad spectrum of patient groups studied in recent trials, we hypothesized that by using meta-regression analysis more knowledge could be obtained on the factors determining the benefit of CRT. Meta-regression is an analysis tool used to examine the relationship between moderating variables and treatment effect using regression-based techniques. In this study, we conducted a comprehensive systematic review, meta-analysis, and meta-regression of data from contemporary randomized controlled trials (RCT) to determine which factors may determine the outcome of CRT.
MATERIALS AND METHODS
Eligibility criteria
We included all RCTs that compared CRT with medical treatment or implantable cardioverter-defibrillator (ICD) alone. We included RCTs that 1) enrolled patients with systolic heart failure with a left ventricular ejection fraction (LVEF) ≤40%, 2) compared CRT with control treatment, 3) studied mainly patients with sinus rhythm, and 4) reported data on clinical events such as death and hospitalization for heart failure. We excluded trials that 1) exclusively enrolled patients with atrial fibrillation, 2) compared CRT with left ventricular (LV) pacing only as the control arm, 3) compared different types of programming (such as simultaneous versus sequential biventricular pacing), and 4) compared different methods of procedure (such as transvenous versus epicardial LV lead placement or triple site versus double site pacing). No restrictions were imposed on the mode of treatment in control groups, etiology of HF, study period, sample size, or publication status.
Data sources and searches
We performed an electronic search of the PubMed, Embase, and Cochrane Central Register of Controlled Trials (CENTRAL) from the inception of each database to October 2013. The electronic search strategy was complemented by a manual review of the reference lists of included articles. References of recent reviews, editorials, and meta-analyses were also examined. One investigator performed the screening of titles and abstracts, identified duplicates, reviewed full articles, and determined their eligibility. This work was subsequently cross-checked by a second reviewer. Disagreement between reviewers was resolved by discussion. The most updated data for each study were searched manually, and chosen for abstraction. Data extraction was independently done by two reviewers and checked by a third reviewer.
Risk of bias assessment
The quality of eligible RCTs was assessed using the Cochrane Collaboration's tool for the risk of bias (19). Both the manuscript and protocol, if available (published or online), were reviewed for relevant information. Risk of bias was assessed by one reviewer and cross-checked by a second reviewer.
Study outcomes and definitions
Independent variables in this study were hard clinical outcomes. The primary study endpoint was all-cause mortality, while the secondary endpoint was hospitalization for heart failure.
Data synthesis and analysis
Odds ratios (OR) with 95% confidence intervals (CI) were presented as a summary statistic. We calculated pooled ORs with the use of the random effects model postulated by DerSimonian and Laird (20). Statistical heterogeneity was assessed with Cochran Q via a chi-square test and was quantified with the I2 test (21). Publication bias was assessed by funnel plot asymmetry and Egger's test.
Exploratory meta-regressions were performed to assess heterogeneous study effects. Covariates that were tested include: 1) QRS duration, 2) QRS morphology, 3) ischemic origin, 4) baseline New York Heart Association (NYHA) functional class, 5) baseline LVEF, 6) LV end-diastolic dimension (LVEDD), and 7) LV end-diastolic volume (LVEDV). QRS morphology was quantified as the proportion of left bundle branch block (LBBB) documented in each trial, excluding those which exclusively enrolled HF patients with a narrow QRS duration. Analysis for NYHA classification was done with the proportion of patients with NYHA functional class III or IV as a covariate. We performed meta-regression analyses using two different statistical models to estimate residual between-trial variance: 1) a random effects model with a restricted maximum likelihood (REML) estimate (22), and 2) a Bayesian random effects model (23).
Subgroup analysis was planned with stratification according to 1) treatment modality of the control groups (ICD vs. medical therapy), 2) NYHA function class (predominantly class I/II vs. III/IV), or 3) follow-up duration (<1 vs. ≥1 yr). Interaction was tested with the use of a mixed-effects meta-regression model (REML method). Sensitivity analysis was done on studies with a low risk of bias. Excluded in the sensitivity analysis were studies with >1 entry assigned to be at high or unclear risk of bias assessed with the Cochrane Collaboration's tool (except for the domains of blinding on patient and physician).
Statistical analysis
Statistical analysis was performed using the "metafor" and "meta-commands" packages in R programming, version 3.0.2 (The R Foundation for Statistical Computing, Vienna, Austria). Results were considered statistically significant if the 2-sided P<0.05. The Bayesian random effects model was constructed with WinBUGS v.1.4.3 (MRC Biostatistics Unit, Cambridge, UK) (24). Odds ratios (OR) with 95% credible intervals (CrIs) are presented as summary statistics, and results for which the CrIs of the ORs did not include one were considered significant. Non-informative prior distributions were selected so as to allow the data to dominate the final results. We ran Markov chain Monte Carlo samplers in WinBUGS, running three chains with different starting values. A burn-in phase of 20,000 iterations was followed by 50,000 updates, where the number of burn-in iterations was chosen according to the Brooks-Gelman-Rubin method for convergence checks (25).
RESULTS
Study selection
Fig. 1 describes the flow of systematic literature review according the Statement of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. Among 785 potentially relevant items, 23 trials comprising 10,103 patients were finally selected for this meta-analysis.
Systematic review and study characteristics
Table 1 briefly describes the key features of the included trials. While many of the studies compared cardiac resynchronization therapy defibrillation (CRT-D) with ICD, some compared cardiac resynchronization therapy pacemaker (CRT-P) with medical therapy. One study enrolled patients undergoing coronary artery bypass graft (CABG) surgery and randomized to CRT-P with CABG or CABG alone (26). Another study compared CRT-D plus bone marrow mononuclear cell transplantation (BMMC) to BMMC alone (27). Two trials had not been published in peer-reviewed journals, so data were extracted from online source (28, 29).
Mean age in the individual studies ranged from 58 to 72 yr, and the proportion of males ranged from 63% to 96%. Mean duration of the QRS complex was highly variable across trials and ranged from 95 ms to 174 ms. Meanwhile, LVEF was uniformly low (21% to 30%). Estimated median duration of follow-up was 14.1 months.
Risk of bias within studies
The risk of bias of each trial was assessed with the Cochrane Collaboration's tool and is summarized in Fig. 2. All of the included studies were described as randomized trials. Allocation concealment was appropriately described in 12 trials, while clinical outcomes were adjudicated under proper blinding in 16 out of the 23 trials. Double blinding was done in 14 trials, while two trials blinded only participating patients but not treating physicians.
All-cause mortality
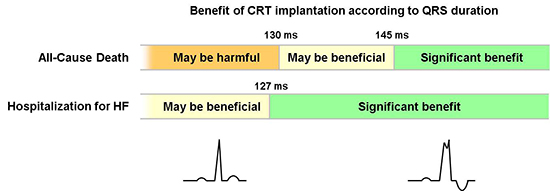
Pooling of the 23 trials with the random-effects model showed a significant benefit of CRT over control treatment in terms of overall survival (OR, 0.82; 95% confidence intervals [CI], 0.68-0.98; P=0.027) (Fig. 3A). There was no significant publication bias (P=0.150 by Egger's test). The effects of CRT varied across trials with small to moderate heterogeneity (I2=25%, P=0.146). Meta-regression analyses were performed with the aim to explore factors explaining the heterogeneity. As shown in Fig. 3B, we found a significant linear association between the benefit of CRT and the length of the QRS duration [log OR=-0.01×(QRS duration)+1.34; P=0.009]. The model incorporating QRS duration as a covariate yielded no residual heterogeneity (I2=0%, P=0.367). There was no effect of CRT in patient with a QRS duration of 130 ms (OR, 1.00; 95% CI, 0.80-1.25). The benefit of CRT was more apparent as QRS lengthened and was statistically significant at a QRS duration ≥145 ms (OR, 0.86; 95% CI, 0.74-0.99). The estimated OR derived from the random-effects meta-regression model was 0.81 (95% CI, 0.72-0.93) for 150 ms. With a QRS duration <130 ms, the model suggested a potential harm with CRT without statistical significance: for example the estimated ORs at a QRS duration of 120 ms was 1.11 (95% CI, 0.83-1.49). The relationship was not significant for any other study variables including QRS morphology, ischemic origin, NYHA functional class, LVEF, LVEDD, and LVEDV (Table 2).
The Bayesian random effects model yielded a wider range of credible intervals. As a result, the pooled OR of CRT compared to control treatment was statistically insignificant (OR, 0.84; 95% CrI, 0.67-1.10). Meta-regression with the Bayesian model showed a similar relationship and slope with wider credible ranges than did the REML estimate model. The ORs estimated from the Bayesian approach were 1.00 (95% CrI, 0.73-1.36) for a QRS duration of 125 ms, and 0.78 (95% CrI, 0.64-1.00) for 156 ms.
Hospitalization for HF
A total of 16 trials comprising 7,511 patients contributed to the analysis for the secondary endpoint, hospitalization for HF. No significant publication bias was present (P=0.113). While CRT was shown to reduce the risk by as much as 41% (OR, 0.59; 95% CI, 0.47-0.74; P<0.001), there was a high degree of heterogeneity between studies (I2=54%, P=0.006) (Fig. 4A). Among a variety of study-level variables, QRS duration best explained the difference between studies (Fig. 4B). The meta-regression showed that the magnitude of risk reduction in HF hospitalization was greater with an increased duration of the QRS complex (log OR=-0.01×[QRS duration]+1.11; P=0.009). According to the model, the estimated ORs were 0.83 (95% CI, 0.62-1.11) for a QRS duration of 120 ms and 0.60 (95% CI, 0.50-0.71) for 150 ms. The shortest QRS duration at which CRT was significantly better was 127 ms (OR, 0.77; 95% CI, 0.60-0.98). The QRS duration where CRT was equivalent to control treatment in terms of HF hospitalization was found to be 103 ms. No other study covariates were significantly associated with the relative efficacy of CRT, while QRS morphology showed marginal significance (P=0.097) (Table 2).
The Bayesian random effects model yielded similar results. The pooled estimate of OR was 0.58 (95% CrI, 0.44-0.75). Meta-regression with empirical Bayesian estimates showed that for QRS durations ≥127 ms CRT significantly reduced the risk of HF hospitalization (OR, 0.74; 95% CrI, 0.50-0.99).
Subgroup analysis
Included trials were divided into two subgroups according to the treatment modality of the control group, i.e. medical treatment or ICD. Two trials were excluded from this analysis because of difficulties determining the precise classification. In one of these trials, the decision to implant CRT-P or CRT-D was left to the discretion of the treating physician, and patients were randomized to CRT-ON or CRT-OFF groups while keeping a double dummy (4). Another trial enrolled patients undergoing BMMC, which cannot be classified as a "conventional" medical treatment (27). Meta-analysis showed that CRT was associated with a significant survival benefit when compared to medical treatment (OR, 0.64; 95% CI, 0.53-0.78; P<0.001) but not when compared to ICD (OR, 0.98; 95% CI, 0.77-1.26; P=0.901, P for interaction=0.024). Notably, the relative efficacy of CRT vs. ICD relied upon the duration of the QRS complex (P=0.002): CRT was better than ICD only when the QRS complex was wide. Meanwhile, the benefit of CRT versus medical treatment was independent of the QRS duration (P=0.271) (P for interaction=0.015).
No significant interactions were found in subgroup analyses for either NYHA function class (P=0.628) or follow-up duration (P=0.626).
Sensitivity analysis
A sensitivity analysis was done for studies with a low risk of bias. Eighteen out of 23 trials met the "low risk of bias" criteria that were defined in this study. The sensitivity analysis generally agreed with the main analysis: the pooled OR was 0.81 (95% CI, 0.67-0.99; P=0.041) for all-cause mortality and 0.60 (95% CI, 0.48-0.75; P<0.001) for HF hospitalization. In addition, meta-regression for trials with low risk of bias also resulted in similar outcomes compared with analyses including all trials (Table 2).
DISCUSSION
In this systematic review and meta-analysis, we found that 1) CRT reduced the risk of all-cause mortality and hospitalization for HF, 2) the benefit of CRT was dependent on the duration of QRS complex, 3) the cutoff value of a QRS duration at which significant benefit was observed differed according to which endpoint of interest was investigated, and 4) the relationship between the advantage of CRT and QRS duration was significant only when compared to ICD, not to medical treatment.
Current guidelines strongly recommend CRT implantation in symptomatic HF patients with sinus rhythm, low LVEF, and a prolonged QRS duration (9, 10). However, there are ongoing controversies regarding specific indications for CRT, among which QRS duration is one of the most debated. Recently, the ACCF/AHA guidelines limited the Class I indication for CRT to patients with a QRS duration ≥150 ms (9, 30). However, a QRS duration of 120-150 ms is still recommended as the Class I indication in the European Society of Cardiology (ESC) guidelines if the patient has an LBBB pattern and depressed LVEF (30). The recent change in the ACCF/AHA guidelines was triggered by evidence from clinical trials where subgroup analyses showed a better response to CRT in patients with a wider QRS duration (≥150 ms) (4, 7, 31, 32). A recent meta-analysis also showed the reduction in adverse events associated with CRT was limited to patients with a QRS duration ≥150 ms, but not evident in patients with a QRS duration <150 ms (11). Contradictory evidence also exists. A post-hoc analysis of CARE-HF, one of the pivotal trials, showed that QRS duration at baseline had no value in predicting unfavorable outcomes (12).
Recent major CRT trials focused on expanding the indications for CRT. The NARROW-CRT and EchoCRT trials studied patients in whom the QRS interval was narrow but intraventricular dyssynchrony was evident on echocardiography (11, 17). The LESSER-EARTH and RESPOND trials also enrolled patients with a narrow QRS complex, but did not require the presence of LV dyssynchrony (15, 16). The rationale of these trials was built on the findings of a discrepancy between dyssynchrony as assessed by echocardiography and QRS duration assessed by electrocardiogram (33, 34). However, these trials showed conflicting results: some were positive (15, 17), while the others were negative including a well-designed large-scale trial (16, 18). They are reflected in this meta-analysis in the marginal benefit of CRT observed and the substantial degree of heterogeneity across trials. The results here are in contrast to previous meta-analyses which clearly showed a significant survival gain with little or no heterogeneity (35, 36). Understanding the source of the wide heterogeneity with a meta-regression method was the primary objective of this study.
To the best of our knowledge, this study is the first systematic study-level meta-regression to explore covariates that explain the benefit of CRT. With the use of the meta-regression method, we were able to identify QRS duration at baseline as the most reliable predictor for hard clinical events after CRT. There was a clear linear relationship between the benefit of CRT and the duration of the QRS complex. This study provides an important new data that highlights the importance of considering QRS duration when selecting patients for CRT implantation. The expected benefit of CRT in patients with a QRS duration ≥150 ms is unquestionable in terms both of all-cause death and HF hospitalization. In patients with a QRS duration between 130-150 ms, the odds for survival tended to be favorable, but is not definitive. However, a risk reduction in terms of hospitalization for HF is still expected for these patients. In the meantime, CRT use in patients with a QRS duration <130 ms showed little advantage, if any, in terms of admission for HF aggravation. Interestingly, this may actually do more harm than good in terms of death from any cause. It should be reminded that periprocedural complications and inappropriate defibrillator shocks may follow CRT implantation (18, 37). We believe this study provides an important insight into the understanding of current CRT trials, and a firm basis to clinical practice guidelines.
The variable effects of a prolonged QRS duration between trials may be explained by differences in the study design. This meta-regression implied the benefit of CRT does not depend on QRS duration when compared to medical therapy. In CARE-HF and COMPANION, in which the control arm was medical treatment, the influence of a prolonged QRS duration was less evident (7, 8). In contrast, MADIT-CRT, and RAFT compared CRT-D versus ICD (31, 32), and in the REVERSE trial, more than 80% of patients received CRT-D (4). These trials revealed a prominent impact of an increased QRS duration on the benefit of CRT.
The major strength of this study is the fact that this is the only existing meta-regression in its true sense. A meta-analysis by Sipahi did analyze relative risks according to QRS duration, but they did not measure actual QRS durations. Instead that study used ranks estimated according to the degree of prolongation among all subgroups (11). In addition, a variety of statistical models performed in this study corroborated the main findings. In statistical terms, REML or Bayes estimates are the preferred methods for meta-regression, as conventional random effects models ignore the imprecision in the between-trial variance estimate (38). The main results here were also confirmed by a sensitivity analysis done with low risk-of-bias trials only after all included trials were thoroughly examined for potential risks of bias with the Cochrane Collaboration's tool.
Caution should be taken in interpreting the negative results of this study, especially regarding LBBB. In the current study, the benefit of CRT had only marginal significance with the proportion of LBBB in terms of HF hospitalization. However, subgroup analyses of major clinical trials and a meta-analysis consistently showed a greater benefit in patients with complete LBBB compared with nonspecific intraventricular conduction delay or RBBB (7, 8, 31, 32, 39, 40). It should be noted that this meta-regression for QRS morphology was limited in several aspects. First, trials with narrow QRS duration were excluded in this analysis (15, 16, 17, 18). As a result, only 7 trials contributed to this analysis so that the statistical power was too low to show statistical significance. Second, the proportions of LBBB in each trial were in too a narrow range. Third, in addition, the 2 trials with the highest weight had a similar proportion of LBBBB (71% in the MADIT-CRT, and 72% in the RAFT) (31, 32).
This study has several limitations. First, this meta-analysis was comprised of 23 randomized trials and inherently shares the limitations of each trial. Two trials included in this analysis have not been peer-reviewed, and several studies were revealed to have a profound risk of bias. However, sensitivity analysis excluding those high risk-of-bias trials validated the main analysis. Second, each study included had a different trial design. The duration of follow-up was profoundly inhomogeneous, and the spectrum of optimal medical treatment evolved drastically over the last 15 yr since the landmark MUSTIC SR trial began enrolling patients (5). To overcome this limitation, we performed several subgroup analyses according to the study design. Third, the benefit of CRT depends not only on baseline patient characteristics, but also on technical factors such as left ventricular lead position or device optimization. However, we still lack data on the optimal protocol or lead positioning except for unfavorable outcomes observed after LV apex positioning (41). These factors were beyond the scope of this study. Fourth, this study was a study-level meta-regression and lacked individual patient-level data which would have permitted a more thorough investigation. Fifth, since multiple testing was done in this study, we cannot exclude the possibility of false positives. Last but not least, the meta-regression associations are observational in nature and should not be interpreted as if they came from randomized comparisons (38).
As a conclusion, CRT compared to control treatment was shown to reduce the risk of all-cause mortality and hospitalization for HF. The relative benefit increased with the prolongation of the QRS duration. This study concludes that patients with a QRS duration ≥150 ms would most benefit from CRT, and patients with a QRS duration <130 ms should not be considered for CRT implantation as it may be potentially be harmful in terms of clinical adverse events.





 XML Download
XML Download