

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gestational diabetes mellitus (GDM) is defined as carbohydrate intolerance with onset or first recognition of pregnancy (1). The prevalence of GDM varies from 2.4% to 22.3% worldwide depending on the population studied and the type of diagnostic test employed (23); and the prevalence of diabetes mellitus (DM) continues to increase worldwide (145).
In Korea, 2% to 5% of all pregnant women reportedly develop GDM (6). GDM contributes to maternal and neonatal morbidity, including gestational hypertensive disorders, fetal macrosomia, shoulder dystocia, and cesarean delivery (78); it also produces a significant burden on the economy (9). GDM is also associated with an increased risk for developing type 2 DM, which ranges from 2% to 70% depending on the population being studied and the length of follow-up (10).
Lifestyle intervention and medication can be used to prevent or delay the development of diabetes in women who have been identified early as having a high risk for diabetes (1112). Therefore, the early identification of DM risk at postpartum is imperative and can be determined by postpartum glucose screening. Consequently, both the American Diabetes Association (7) and American College of Obstetricians and Gynecologists (13) recommend postpartum glucose tolerance testing in women with GDM. However, rates of postpartum glucose screening are suboptimal, which range from 18% to 57% (14151617181920).
Asian ethnicity is a well-recognized risk factor for the development of GDM (2122) and more likely to complete postpartum glucose screening than Caucasian women (172324). Therefore, the Asian population is a good candidate to determine clinical and physiological factors that predict and/or contribute to postpartum glucose screening compliance. However, studies available in the context of postpartum glucose testing compliance include Asians as a minor population. In light of this, the present study was conducted to investigate postpartum glucose testing rates in patients with GDM and to determine factors affecting testing non-compliance in the Korean population.
MATERIALS AND METHODS
Study population
This was a retrospective study involving patients with GDM, which was conducted in 4 tertiary centers in Korea between January 1, 2008 and August 31, 2011. Patients who received prenatal care and delivered at the 4 tertiary centers were enrolled in this study. Patients with pre-gestational diabetes were excluded.
Information collected
Demographic, medical, and physiological data were gathered from the women enrolled in this study. We evaluated the age, education level, parity, previous diagnosis of GDM, previous delivery of large for gestational age babies, a history of DM in first-degree relatives, height and weight during the course of pregnancy, gestational age at delivery, pharmacotherapy for GDM during pregnancy, complications of pregnancy (i.e., preeclampsia), birth weight, neonatal intensive care, delivery mode, and postpartum glucose screening.
The pre-pregnancy body mass index (BMI) was calculated for each patient as the weight in kilograms divided by height in square meters. Weight gain was defined as weight at the time of admission for delivery minus the pre-pregnancy weight. The causes for referral were also obtained from patient medical records. Patients were classified based on referral cause (i.e., referral for GDM treatment or for reasons other than GDM treatment).
Diagnosis of GDM
All pregnant women were screened for GDM either at 24-28 weeks of gestation or entry to prenatal care when risk factors for diabetes were present using a 1-hr 50-g oral glucose challenge test. Risk factors that contributed to early screening included a history of GDM; having a first-degree relative with diabetes; a history of having a macrosomic, stillborn, or anomalous infant; and a pre-pregnancy BMI >25 kg/m2 (25).
Women with glucose levels ≥ 140 mg/dL underwent a standard 3-hr 100-g oral glucose tolerance test. The diagnosis of GDM was based on the criteria by Carpenter and Coustan and at least 2 out of the following 4 diagnostic criteria had to be fulfilled: fasting plasma glucose ≥95 mg/dL, and 1-, 2-, and 3-hr glucose levels of ≥180 mg/dL, ≥155 mg/dL, and ≥140 mg/dL, respectively (24).
Management of GDM
Out of the 4 tertiary centers, 3 centers (centers 1, 2, and 3) implemented a multidisciplinary team approach with diverse healthcare professionals (i.e., obstetricians, endocrinologist, and dieticians). After the diagnosis of GDM, all patients visited an endocrinologist to monitor and control their blood glucose levels. However, center 4 used traditional methods where blood glucose was monitored and controlled by obstetricians. All centers provided similar care for patients with GDM, including healthy dietary practices, weight management, exercise, monitoring lifetime risk of diabetes, postpartum glucose screening, and periodic reevaluation of glucose tolerance.
Postpartum glucose test
Postpartum glucose testing was conducted using a 2-hr 75-g oral glucose tolerance, fasting glucose, or hemoglobin A1C (HbA1C) test. Postpartum glucose test results were categorized as normal, pre-diabetes (i.e., impaired fasting glucose and/or impaired glucose tolerance), and diabetes. The diagnostic criteria for pre-diabetes and diabetes were based on the American Diabetes Association guidelines (26). Diabetes was defined as HbA1C level of ≥6.5%, fasting glucose level of ≥126 mg/dL, 2-hr plasma glucose level of ≥200 mg/dL post-75 g glucose challenge, or a random plasma glucose level of ≥200 mg/dL with symptoms (i.e., polyuria, polydipsia, and unexplained weight loss). Pre-diabetes was defined as HbA1C level 5.7%-6.4%, fasting glucose level of 100-125 mg/dL (indicating impaired fasting glucose), or a 2-hr glucose level of 140-199 mg/dL post-75 g glucose challenge (indicating impaired glucose tolerance).
Statistical analysis
Data were expressed as the mean±standard deviation for continuous variables and percentages for categorical variables. Student's t-tests were used to assess the statistical significance between normally distributed continuous variables. Categorical variables were compared using the chi-square test. A model of multivariate logistic regression analysis was used to evaluate the factors related to postpartum glucose screening non-compliance after adjustment for covariates that had statistical values of P less than 0.15 in the univariate analysis. Results were considered statistically significant when P values were <0.05 (two-sided). Statistical analyses were performed using SPSS software, version 12.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
A total of 1,686 patients with GDM were included during the study period. The mean postpartum glucose testing rate was 44.9% (757/1,686 patients). Based on the oral glucose tolerance test results, 172 (31.2%) had prediabetes, and 54 (9.8%) had diabetes. Based on the fasting glucose results, 82 (35.5%) had prediabetes, and 6 (2.6%) had diabetes. In contrast, using HbA1C test, 165 (43.5%) had prediabetes, and 91 had diabetes (24.0%). With the combination of oral glucose tolerance, the fasting glucose and HbA1C test, 334 (44.1%) had prediabetes, and 139 had diabetes (18.4%).
The characteristics of the study participants are shown in Table 1. Patients who were non-compliant to postpartum glucose testing had a higher parity and weight gain during pregnancy compared to women who were compliant to postpartum glucose testing. The incidences of preterm birth and preeclampsia were higher in patients who were non-compliant to postpartum glucose testing compared to women who were compliant to postpartum glucose testing. Patients who were non-compliant to postpartum glucose testing were more likely to be referred from private clinics and less likely to have used pharmacotherapy. However, other characteristics that were evaluated in this study were not different between the 2 groups.
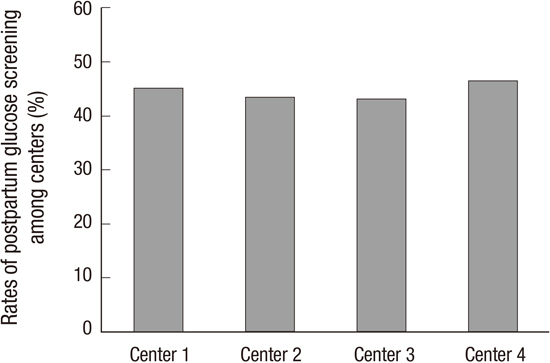
There were no differences in the risk factors that contributed to early screening between women who were and were not compliant to screening (Table 2). Furthermore, there was no difference in the postpartum glucose testing rate among the 4 centers (P=0.716, Fig. 1).
We evaluated the factors related to postpartum glucose screening non-compliance by using multivariate logistic regression analysis. According to the multivariate analysis, patients with high parity, larger weight gain during pregnancy, and referral from private clinics due to reasons other than GDM treatment were less likely to receive postpartum glucose testing. However, patients with pharmacotherapy for GDM were more likely to be screened (Table 3).
DISCUSSION
The postpartum glucose testing rate in this study was 44.9% (757/1,686 patients), which is comparable to results from other studies (16). Several studies that were conducted to evaluate independent factors related to postpartum glucose screening compliance in various racial/ethnic cohort groups reported that the Asian group was associated with higher postpartum glucose screening rates (172324). These rates (45%-85%) were higher than the rates from our study population which included only Asian participants. According to these results, the differences in screening rates may be due to the variations in how postpartum glucose screening was recommended by the health care providers to Asian women compared to other racial/ethnic groups and not based on the idea that Asians seek more healthcare given their higher prevalence of diabetes (27).
We identified factors associated with low postpartum glucose screening testing rates. According to the results, patients who were transferred to the center due to reasons other than GDM treatment underwent less frequent postpartum glucose screening tests. Although the precise reason for this association was uncertain, it has been previously reported that women who attended postpartum visits were more likely to complete postpartum glucose screening (1617232428). There is a high possibility of discontinuing antenatal and postpartum care in referred patients (i.e., referred and delivered at a tertiary center and then referred back to the private clinic after delivery) indicating that referred patients may not attend postpartum visit. It is possible that these patients may have completed postpartum glucose screening at the private clinics, thereby did not return to the tertiary center for postpartum care. However, Russell et al. (17) reported that women attending postpartum visits at hospital-based clinics were twice as more likely to completing postpartum glucose testing compared to women at community clinics. Moreover, there is a high possibility of omitting postpartum glucose screening at the private clinics due to physician's limited access to the patient's antenatal medical information regarding gestational diabetes or lack of vigilance (8). Therefore, these disturbances in medical care from the prenatal to postpartum periods in referred patients may contribute to the low rates of postpartum glucose screening. GDM is associated with various maternal and fetal complications, such as preeclampsia and large for gestational age babies (78). Therefore, patients with GDM should be referred to tertiary centers for appropriate treatment where they should be informed regarding postpartum glucose screening during pregnancy and provided reminders for the screening tests (29).
Compatible to findings from other studies, patients who were non-compliant to postpartum glucose screening had higher parity (14161924) and were less likely to require insulin for glycemic control (16192024). Moreover, patients who were non-compliant to postpartum glucose screening had a higher weight gain during pregnancy. This may be a reflection of the "healthy cohort" effect where individuals who are more health-conscious and made efforts to gain less weight during pregnancy are more likely to seek treatment or follow-up (30).
It has been found in a previous study that a multidisciplinary team approach of caring for patients with DM resulted in large improvements in patient management (31). Similarly, Berg et al. (32) reported an improvement in GDM outcome by using a multidisciplinary team approach and Sempowski and Houlden (33) recommended referrals to multidisciplinary teams for intensive glucose control for patients with GDM. It has been reported that visits with an endocrinologist after delivery are associated with better screening rates (28). Although centers 1, 2, and 3 in this study implemented a multidisciplinary team with obstetricians, endocrinologist, and dieticians while center 4 included only obstetricians, we did not observe any differences in postpartum glucose screening rates among these centers. Further studies are needed to evaluate these unexpected results.
Out of 757 women who underwent postpartum glucose screening in this study, 18.4% patients had diabetes, which was higher compared to results from other studies. According to previous reports, the prevalence of diabetes ranged 1%-8% in Caucasians (14161724). In contrast, our results were comparable to results published by Jang et al. (34) who reported that approximately 15.1% of 311 Korean women had diabetes. These discrepancies between studies may be partially due to the higher prevalence of DM in the Asian population (3536).
Some limitations should be kept in mind when interpreting our findings. As our study was confined to medical chart review, we could not determine physician dependent factors including frequency of physician contact, use of reminder system and time spent on educating the consequences of GDM, which were associated with non-compliance to postpartum glucose testing. Further studies are needed to examine physician dependent factors for improvement of compliance to postpartum glucose testing.
In conclusion, 55.1% of patients with GDM failed to return to the tertiary center to complete postpartum glucose testing in this study. Considering the high prevalence of DM (18.4%) during the postpartum period in our study population, it seems urgently necessary to educate patients regarding the factors affecting non-compliance and the importance of postpartum glucose testing. Furthermore, patients who are referred from other private clinics should be encouraged for postpartum glucose testing and a collaborative strategy to enhance continuity of care and to alert patients of follow-up testing should be implemented.



 XML Download
XML Download