

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Prostate cancer (PCa) patients can be stratified into different risk groups in terms of predicting prognosis and determining treatment strategy (1). Although the early detection rate of PCa has recently increased due to prostate-specific antigen (PSA)-based screening (2), the number of intermediate-risk (IR) and high-risk (HR) cases at an elevated risk of biochemical recurrence (BCR) and disease progression compared to those with low-risk (LR) still make up more than half of newly diagnosed cases (2). The benefits of radical prostatectomy (RP) as first-line treatment for IR and HR PCa as monotherapy or part of a multimodal plan are achievement of excellent local control, accurate pathological staging and guiding additional therapy based on better prediction of prognosis (34).
Radical perineal prostatectomy (RPP) has been used for much of the 20th century as the oldest radical procedure for treatment of PCa (5). Although RPP use decreased after nerve-sparing radical retropubic prostatectomy (RRP) was first described in the 1980s, there has recently been a renewed interest in RPP (6), which is an effective minimally invasive technique with rapid recovery (67), minimal cost (8) and the ability to be quickly mastered due to relatively easy dissection and anastomosis of the urethra (67). The surgical outcomes of RPP with nerve-sparing and extended radical modifications are very similar to those of other RP series (678910). However, as pelvic lymph node dissection (PLND) is conventionally recommended in patients with IR or HR PCa (11), RPP is typically offered only to patients with LR PCa, in whom the risk of lymph node involvement (LNI) is < 1% (12) due to a separate skin incision for PLND.
However, the indications for PLND and the effects of PLND on oncological outcomes of PCa remain unclear. There has been a significant decline in the use of PLND following the introduction of minimally invasive RP (MIRP) (13). Additionally, in the era of PSA testing, PLND is less often indicated during RP due to the significantly decreased incidence of LNIs, thereby making avoidance of RPP no longer valid (14). Stage migration in the recent PSA era has dramatically reduced the incidence of LNI to 1% (14). Up to date, no consistent conclusions have been reached regarding the role of PLND in improving oncologic outcomes for IR and HR patients (15). With a resurgence of interest in the perineal approach, it is critical to determine whether RPP is effective for cancer control in patients with IR or HR disease who would be most likely to benefit from RP, but in whom PLND is generally recommended. The goal of the present study was to investigate the oncologic efficiency of RPP as a first-line treatment in patients with IR or HR PCa by making a direct comparison of pathological and oncologic outcomes among IR and HR PCa treated either by RPP, RRP, and MIRP in a single institution.
MATERIALS AND METHODS
Clinico-pathological characteristics and onco-surgical outcomes were retrospectively reviewed in IR and HR PCa patients. From 1995 through 2013, we identified 2,581 consecutive patients undergoing RP for IR (cT2b-T2c, bGS=7, or PSA 10-20 ng/mL, n=1,377, 53%) and HR (≥cT3, bGS 8-10, or PSA >20 ng/mL, n=1,204, 47%) PCa at Samsung Medical Center (16). Of these, 689 (26.7%), 402 (15.6%) and 1,490 (57.7%) underwent RPP, RRP and MIRP (laparoscopic radical prostatectomy [LRP], n=206; robot-assisted laparoscopic radical prostatectomy [RALRP], n=1,284), respectively. Patients who received neoadjuvant treatment (i.e., hormonal therapy or radiation therapy) were excluded from this study. The number of surgeons performing RRP, LRP and RALRP was 4, 1, and 4, respectively, while RPP was performed by only one surgeon.
Clinical stage was assigned according to the 2009 TNM system. All patients were preoperatively staged for metastases with a bone scan, magnetic resonance imaging (MRI), and pelvic computed tomography (CT). In RPP cases, PLND was performed for accurate diagnosis of LNI via mini-laparotomy (17) or a laparoscopic approach (18) in patients with radiographic findings suspicious for pelvic LNI. Prostatectomy specimens were reviewed with respect to pathologic GS (pGS), pathologic T (pT) stage, and surgical margin (SM) status. Additionally, we deemed men with a pGS of <8 or ≤pT3a PCa to have favorable disease, and those with pGS 8-10 and ≥pT3b or N1 disease to have unfavorable pathologic findings (19). Postoperative incontinence was evaluated by measuring the number of pads used per day. If the patient had no urinary leakage or required only a security pad, this was defined as being continent. In general, patients were followed for recurrence postoperatively using PSA levels and clinical assessment at 3-6-month intervals for the first 3-5 yr, and then annually thereafter. When clinically indicated after surgery, further diagnostic testing was used, including CT, MRI, chest radiography, and/or bone scans. BCR was defined as the first occurrence of two consecutive PSA level rises of >0.2 ng/mL at least 3 months after RP, and distant metastases was defined as a demonstrable metastatic deposit on imaging. PCa-specific survival (CSS) refers to the time from RP to death attributed to PCa or complications related to this disease. Adjuvant treatment was started within 6 months of the surgery, and salvage treatment was started in patients with BCR or clinical progression that were more than 6 months out from RP.
Differences in the clinico-pathologic features based upon surgical technique were assessed using the rank-sum test and chi-square or Fisher's exact test. To evaluate the impact of RP on BCR-free survival (BFS), metastasis-free survival (MFS), and CSS in IR and HR patients, Kaplan-Meier analysis was performed along with log-rank tests. A multivariate proportional hazard regression model was used to identify independent predictors of BCR and metastases. All P-values were two-sided and P<0.05 was considered to be statistically significant. The analyses were performed using SPSS commercial software, version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Table 1 lists the clinical and pathologic patient characteristics according to surgical approach. The HR feature was observed in 40.3%, 46.8% and 49.5% of men undergoing RPP, RRP and MIRP, respectively (for a pairwise comparison of RPP vs. RRP, P=0.04; RPP vs. MIRP, P<0.001). PLND was performed in 7.1%, 21.4% and 19.3% cases of RPP, RRP and MIRP, respectively (P<0.001). The rate of neurovascular bundle preservation was significantly higher in MIRP (67.3%) than RPP (56.2%) and RRP (29.9%) (P<0.001). In addition, estimated blood loss was lower in RPP patients compared to RRP patients (P<0.001) although higher compared to the MIRP group (P<0.001). There were statistically significant differences between continence rate at 1 yr (RPP, 85.8%; RRP, 70.9%; MIRP, 76.6%, P<0.001).
RPP patients had significantly lower proportions of ≥pT3 stage and higher proportions of pGS ≥8 compared to MIRP patients (P=0.002 and P=0.047) although there was no statistically significant difference between the three cohorts with respect to proportion of unfavorable disease (RPP, 5.1%; RRP, 5.7%; MIRP, 4.0%, P=0.21) (Table 1). While there were significantly fewer positive SMs with MIRP for pT2 organ-confined disease (RPP, 17.5%; RRP, 17.8%; MIRP, 8.8%, P<0.001), we found no significant difference in the incidence of positive SMs among men with extra-prostatic extension and seminal vesicle invasion irrespective of surgical approach (RPP, 41.9%; RRP, 44.4%; MIRP, 40.0%, P=0.55).
There was a significant difference in median follow-up duration between the RPP, RRP and MIRP groups (RPP, 68; RRP, 42; and MIRP, 33 months; RPP vs. RRP, P<0.001; RPP vs. MIRP, P<0.001) (Table 1). During the follow-up period, a total of 443 patients experienced BCR, 156 (24.7%) in the RPP group, 90 (24.7%) in the RRP group, and 197 (14.1%) in the MIRP group (Table 1). Distant metastasis was detected after RP in 5.1% of RPP, 1.7% of RRP and 2.4% of MIRP.
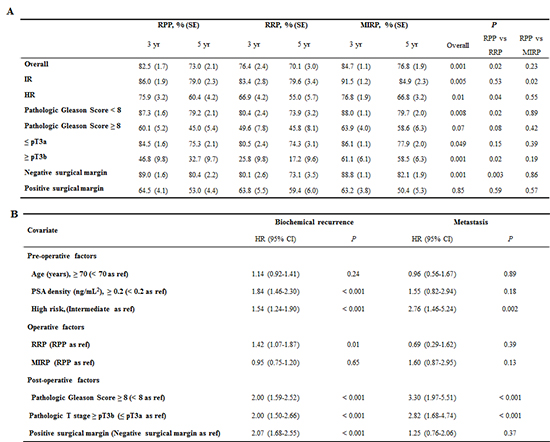
In terms of the BFS rate, RPP appears to be significantly better than RRP and on par with MIRP. BFS rate at 5 yr was 73.0%, 70.1% and 76.8% for RPP, RRP and MIRP, respectively (RPP vs. RRP, P=0.02; RPP vs. MIRP, P=0.23) (Table 2). Importantly, in HR PCa, RPP was associated with higher BFS rates compared to RPP (P=0.04), but comparable BFS rates were demonstrated between RPP and MIRP (P=0.55). Similarly, there were no significant differences in BCR between RPP and MIRP when stratified by pGS, pT stage and SM positivity (Table 2). The comparison of MFS rates according to surgical approach also demonstrated no meaningful difference in overall cohorts and in subgroup analysis stratified by pre-operative risk (Fig. 1).
The independent prognostic factors associated with BCR and metastases were statistically analyzed using the multivariate Cox proportional hazards regression method (Table 3). After adjusting for age, PSA density, pGS, pT stage, and SM status, the stratified preoperative risk were shown to be significantly associated with oncologic outcomes (BCR, hazard ratio=1.54, P<0.001; metastases, hazard ratio=2.76, P=0.002). While PSA density, pGS, pT stage, and SM status (all P<0.001) were significant predictors of BFS, independent factors of MFS included pT stage (P<0.001) and pGS (P<0.001), suggesting that the presence of unfavorable pathology defined by high pGS (≥8) and advanced T stage (≥pT3b) was significantly associated with increased risk of BCR and distant metastasis from PCa. Surgical modality did not predict MFS in multivariate regression models controlling for these cofactors while RRP was associated with increased BCR (HR 1.44, P=0.01) compared to RPP.
In landmark survival analyses in RPP (Table 4), the 10-yr MFS and CSS rates for the entire cohort in patients who underwent RPP were 87.1% (IR, 93.2; HR, 77.5%, P<0.001) and 92.8% (IR, 94.0; HR, 89.3%, P=0.13, Fig. 2A, B), respectively. In RPP, 10-yr MFS and CSS rates were also better for those with a pGS <8 (Table 4 and Fig. 2C) and <pT3b disease (Table 4 and Fig. 2D), and these differences were also statistically significant (all P<0.001). Finally, favorable RPP pathology was associated with improved oncologic outcomes in the overall cohort (MFS, 93.3% and CSS, 94.4% at 10 yr, all P<0.001) (Table 4).
DISCUSSION
By far the most common argument put forward in favor of a retropubic approach as opposed to RPP is the issue of PLND, since LNs can be dissected via the same skin incision or port sites. In this context, RPP has typically been offered to patients with LR PCa in whom PLND is unnecessary (12); therefore, there is limited evidence in support of RPP in IR and HR patients in whom PLND is recommended. As for PLND, improved imaging techniques and accurate LNI risk discrimination could help to better guide the clinician in deciding whether PLND is required, and as a result, unnecessary PLND can be avoided. Because of limited comparing studies between RPP and other RP procedure regarding surgical outcomes, it is difficult to determine the best approach against IR and HR PCa.
Since the opening of the Samsung Medical Center in 1994, RPP has been widely performed in addition to RRP, LRP and RALRP. In this study reporting a large single institutional experience of surgical efficacy of RPP, RRP, and MIRP in patients with IR and HR PCa, we found no difference in disfavor of RPP regarding short-term oncologic outcomes in IR and HR patients, demonstrating comparable oncologic outcomes with previous reports (20212223). Furthermore, HR and the final pathologic characteristics rather than surgical approach were significant predictors of disease recurrence. Finally, survival outcomes of RPP in clinically HR PCa patients (a 10-yr MFS, and CSS of 77.5% and 89.3%, respectively) are comparable with those of other RRP and MIRP reports, although published data for RP in HR PCa patients are very heterogeneous in terms of risk criteria, final pathology, adjuvant/salvage treatments, and follow-up duration (2425).
The incidence of positive SMs in this study was comparable to those found in recent studies (2627). Especially, the margin positivity rate was similar between RPP, RRP, and MIPR in HR PCa, and previous open and MIRP series reported positive SM rate ranges from 21% to 47% (28). The improved MIRP SM status in LR disease may be attributed to better visualization of the prostate capsule and apex secondary to magnification, fiber-optic illumination, and CO2 insufflation that tamponades venous bleeding (29). Lower estimated blood loss during MIRP than other RP techniques could be due to high intra-abdominal pressure during pneumoperitoneum for MIRP procedures (23).
We recognize that our study is limited by its retrospective design. As the application of additional therapies is not standardized, the exact effects of RP as a monotherapy for IR and HR PCa could not be determined in our series. Further long-term studies evaluating functional outcomes focusing on post-operative potency are required to better compare pros and cons of various RP approaches.
To our knowledge, the present study is the largest single-institution series to investigate the impact of three different approaches on onco-surgical outcomes following RP for patients with IR and HR PCa. Taken together, our results support the use of RPP as an attractive alternative surgical approach in these patients, as it achieves equivalent favorable oncologic outcomes when applied alone or in combination with other therapies.



 XML Download
XML Download