

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Compared to other etiologies, patient and graft survival rates are relatively poor for hepatitis C virus (HCV) related liver transplantation (LT) due to universal HCV recurrence after LT and progressive fibrosis (12345). To date, the absence of preventive strategy for HCV reinfection after LT is a major challenge for HCV recipients undergoing LT (6). For best efficacy of anti-HCV treatment, pre-emptive or early post-transplant antiviral therapy should be initiated soon after LT, optimally within 1 month when the viral load is at its lowest level and fibrosis is absent (78). However, in the early post-transplant period, antiviral therapy may be less effective due to high level of immunosuppression. In addition, there is a high risk of poor hematological tolerance, rejection, and sepsis in the early post-transplant period (789101112). Although recent direct acting antivirals represent a new era in HCV associated liver disease, individual centers are now reporting their experience with the new agents in the post-transplant period (51314). Therefore, the current 'standard of care' for HCV recurrence in recipient is still pegylated interferon and ribavirin for 48 weeks irrespective of viral genotype (213).
We designed the present study with the following aims: 1) to evaluate the result of early protocol biopsies in HCV related recipient after LT; 2) to investigate the result of response-guided standard antiviral therapy for HCV recurrence based on early protocol biopsy after LT. In the present study, HCV related liver disease or HCV infection was confined as in case of positive serum HCV-RNA. HCV recurrence after LT was defined as recurrence of serum HCV-RNA positivity after LT.
MATERIALS AND METHODS
Immunosuppressive protocol after LT
All recipients had received induction with 20 mg of intravenous basiliximab (IL-2 receptor antagonist) within two hours before LT and on postoperative day 4. Basal immunosuppression was based on triple immunosuppressive regimen with calcineurin inhibitor (mostly, tacrolimus), mycophenolate mofetil and steroids. Tacrolimus or cyclosporine was started within 5 days after LT. Tacrolimus and cyclosporine doses were adjusted according to individual clinical need with respective target whole blood trough levels around 8-12 ng/mL and 200-300 ng/mL for the first month after LT, followed by 5-8 ng/mL and 100-200 ng/mL thereafter. Mycophenolate mofetil was started at 1.0 g daily within 5 days (500 mg twice a day) for most patients, and adjusted according to the occurrence of related side effects. Intravenous methylprednisolone 500 mg was given intra-operatively before portal perfusion. It was tapered from 200 mg to 20 mg within 6 days. Thereafter, oral prednisolone was continued at 20 mg daily. It was tapered to 0-5 mg/day until 6 months post-LT.
Outpatient follow-up were usually conducted once a week for the first month after discharge, and was gradually lengthened to every 3 or 4 months, with additional visits as clinically necessary. A complete laboratory investigation, including liver function tests and blood calcineurin inhibitor trough level, was conducted at each follow-up.
Laboratory testing
HCV-RNA test and genotyping was performed using molecular methods. HCV-RNA was quantitatively measured using serum (gel EDTA bottle) by real-time reverse transcription polymerase chain reaction (detection range, 12-100,000,000 IU/mL). HCV genotyping was performed using serum (gel EDTA bottle) by polymerase chain reaction and hybridization (detectable patients in case of ≥500 IU/mL HCV-RNA; detectable genotype: 1a, 1b, 2, 3, 4, 5, 6).
HCV-RNA measurement was performed before discharge and at almost every month after LT. In patients who underwent HCV treatment after LT, the assessments included HCV-RNA at baseline, week 4, 12, 24, the end of treatment, and 24 weeks after the end of treatment irrespective of genotype. HCV genotype was usually performed once before LT.
Protocol liver biopsy after LT
Application of early protocol biopsy was confined to HCV recurrence after LT. Protocol biopsies were performed between postoperative day 7 and 14, and at 3±1, 6±1, and 12±1 months after LT with annual biopsies thereafter in HCV related recipients since January 2010. Sono-guided fine needle aspiration liver biopsies were performed by specialized radiologists. The biopsy specimens were stained with hematoxylin-eosin and Masson trichrome. Pathologic reviews were performed by two hepatopathologists at the institution. Hepatic fibrosis was assessed on a four-point scale using the METAVIR system (15). In all cases, an informed consent was obtained from each patient before biopsy.
Patient selection
We retrospectively analyzed the results of protocol biopsies in HCV related recipients who underwent LT at our institute from 2010 to 2012. A total of 510 patients underwent LT during the period, of which 41 were HCV related (8.0%). We excluded patients who had the following: death before protocol biopsy, refusal of biopsy or poor adherence, advanced hepatocellular carcinoma with invasion of major vessels before LT, hepatocellular carcinoma recurrence after LT, re-LT, and no recurrence of HCV after LT. In the present study, we excluded the results of biopsies which were performed during or after HCV treatment.
After LT, 97.6% of HCV related recipients experienced HCV recurrence (n=40). Among the 40 recipients with HCV recurrence, 28 (68.3%) underwent early protocol biopsies more than once within 1 yr after LT. After excluding hepatocellular carcinoma recurrence (n=3), a total of 25 patients were included in the present study.
Response-guided antiviral therapy
The indication of HCV treatment was based on biopsy and laboratory test as shown in the following: 1) any degree of fibrosis related with HCV infection on histology, 2) inflammation degree with more than moderate or HCV hepatitis accompanying with abnormal liver function test. We started standard treatment with pegylated interferon and weight based ribavirin. We adjusted treatment period according to individual response regardless of pre-LT HCV treatment. Definitions of virological response were based on the '2009 AASLD guidelines' (16). In case of rapid virological response (RVR), we treated the patients for 24 weeks after the initial treatment regardless of the genotype. For complete or partial early virological response (EVR), we treated the patients for 48 weeks. In case of breakthrough after RVR or EVR, we treated patients for 72 weeks after the initial treatment. For patients who showed non-tolerance, non-adherence, or non-responder, we discontinued the treatment. The end-point of treatment was the sustained virological response (SVR). In case of relapse, we restarted HCV treatment for 48 weeks unless the patient had been non-tolerant or non-adherent. The end-point of retreatment was also the SVR.
End-points
The primary end-point of the present study was at 12 months after LT, that is, at the time of completion of early protocol biopsies. The secondary end-point was at 24 weeks after completion of HCV treatment for evaluating SVR or relapse, or at the time of discontinuation of HCV treatment due to non-tolerance, non-adherence, or non-responder.
Statistical analysis
Continuous data were presented as mean±standard deviation. Categorical parameters were presented as number of cases with percentage in parenthesis. Continuous variables were compared using Student's t-test. Categorical variables were compared using Pearson's chi-square test or Fisher's exact test. Statistical analyses were performed using SPSS version 19.0 (SPSS Inc., Chicago, IL, USA). All P values were two-sided, and P<0.05 was considered statistically significant.
RESULTS
Demographics
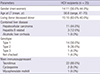
The demographics of the 25 patients used in the present study are summarized in Table 1. Mean age was 56.64±8.09 (range, 41-70) yr, including 15 (60.0%) living donor LT. The 25 patients included 14 (56.0%) patients with genotype 1 and 9 (36.0%) patients with genotype 2. Tacrolimus was the main immunosuppressant (88.0%). The mean follow-up was 43.1 (range, 23-55) months after LT.
Result of early protocol biopsies
Result of early protocol biopsies in HCV related recipient after LT is shown in Fig. 1. Among 20 patients who underwent protocol biopsy at 3, 6, and 12 months post-LT, 7 (35.0%), 10 (76.9% of untreated patients), and 3 (37.5% of untreated patients) came in for HCV treatment, respectively. Based on early protocol biopsies, 20 (80.0%) of 25 patients started treatment for HCV recurrence within 1 yr after LT, including 17 (68.0%) patients within 6 months after LT and 7 (28.0%) patients within 3 months after LT.
Outcome of response-guided therapy for HCV recurrence
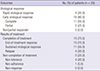
The outcome of response-guided therapy for HCV recurrence after LT is shown in Table 2 and Fig. 2. There was no non- or partial responder in our cohort. RVR was observed in 4 (20.0%) patients. EVR was in 16 (80.0%) patients. RVR plus complete EVR was observed in 15 (75.0%) patients. Among the 20 patients who started HCV treatment, 15 (75.0%) who completed the treatment all showed end-of-treatment response (ETR). However, 5 (25.0%) patients had to discontinue the treatment due to non-tolerance (n=4) or non-adherence (n=1). As the results, of the 20 patients who started HCV treatment, SVR was observed in 11 (55.0%) and relapsed in 4 (20.0%).
According to genotype, SVR was observed in 5 (41.7%) of 12 genotype 1 patients and 6 (75.0%) of 8 non-genotype 1 patients. Regarding genotype 2, SVR was observed in 6 (85.7%) of 7 genotype 2 patients and 5 (38.5%) of 13 non-genotype 2 patients. Even though SVR tended to be higher in non-genotype 1 (75.0%) or genotype 2 (85.7%), there were no significant statistical differences between the results according to genotypes (P=0.197 for genotype 1, P=0.070 for genotype 2). All 4 patients with RVR had genotype 2 infection.
Among 20 patients who underwent HCV treatment, 15 patients (75.0%) maintained negative HCV-RNA until the last follow-up. Every patient is alive until the last follow-up. Overall 3-yr survival rate was 100.0% in 25 patients who underwent protocol biopsies.
Outcome of retreatment after relapse
As shown in Fig. 2, 4 patients who were relapsed started retreatment for HCV. As the results, all patients showed RVR (n=1) or EVR (n=3) and completed retreatment with positive ETR. Two patients achieved SVR (50.0%), and other two were relapsed again.
Predictors for treatment response
Results of univariate analysis of predictors for treatment response are shown in Table 3. Patients who underwent HCV treatment were divided into SVR group (n=11) or non-SVR group (n=9). Only RVR or complete EVR showed significant difference (100% in SVR group vs. 55.6% in non-SVR group, P=0.026). Except this, there was no significant difference or predictor between the two groups, including genotype.
DISCUSSION
Treatment for HCV recurrence after LT is challenging due to lower response compared to non-transplant setting (4). Unfortunately, only one-third of treated recipients achieve SVR when they are treated after LT (23471718192021). Furthermore, antiviral treatment is associated with poor tolerability which frequent needs dose adjustment due to adverse events in recipients (322). In systematic reviews, dose reductions of ribavirin and/or pegylated interferon were necessary for around 70% of patients, and rate of treatment cessation was around 30% (71720). In our study, similar results were obtained, with dose reductions in 80% and treatment cessation in 25%.
Optimal timing of treatment for HCV recurrence after LT together with immunosuppression and new antiviral drugs are of interest (23). In HCV recurrence after LT, there is a trend toward greater recurrence rate of HCV, particularly during the first year after LT (24). Gelley et al. reported that HCV recurrence was observed mainly within the first year after LT (83%), compared to 56% within 6 months and 20% within 3 months (25). However, due to the lack of clinical benefit and occurrence of side effects, there is currently no evidence to recommend prophylactic or pre-emptive HCV treatment to prevent HCV recurrence after LT (2223262728). Directed HCV therapy after histological evidence of HCV recurrence is the mainstay of management for HCV after LT (23). Therefore, in the present study, we designed these directed and response-guided HCV treatment based on early protocol biopsies at 3, 6, and 12 months after LT in selected patients who showed positive pre- and post-LT HCV-RNA. After early protocol biopsies, more than two-thirds of patients (68.0%) started HCV treatment within 6 months after LT and 85.0% of patients started HCV treatment within 1 yr after LT.
With our treatment strategy, the patients showed excellent early on-treatment response (75.0% of RVR or complete EVR) and relatively high SVR rate (55.0%). HCV genotype is one of the most important predictors of HCV treatment response. Among the genotypes, genotype 1 is the most prevalent worldwide and related to a lower response to treatment (13). In Korea, the most prevalent genotype is genotype 1 (41%-53%), followed by genotype 2 (38%-45%) (2930). In the present study, genotype 1 (56.0%) was the most prevalent, also. Even with a high rate of genotype 1 in our study, SVR rate was present in 55.0%, which was higher than that of other studies (23471718192021). These encouraging results might be related to the prevalent favorable IL-28B polymorphism in Korean. About 90% of Korean population had rs12979860 CC type (favorable IL-28B) (31323334). Although our study is lack of IL-28B genotype data, this may be the main reason behind the good result of our cohort.
In addition to IL-28B genotype of donor and recipient, known favorable predictors include younger donor age, lack of severe fibrosis, lack of insulin resistance, low pre- and early post-LT HCV-RNA levels, lack of HIV co-infection, early on-treatment response (RVR or EVR), adherence to drugs or therapy, reduced time since LT, and cyclosporine (1510353637). Among those predictors, for immunosuppressant, some studies have reported higher rates of SVR in patients treated with cyclosporine. However, that is still a matter of debate (4). In the present study, only early on-treatment response was a significant predictor of SVR (Table 3). Contrary to our expectations, genotype 1 or 2 was not significant predictors of SVR (P=0.197 and 0.070). We cannot be sure why genotype was not significant predictor of treatment response. The small number of patients (n=20) in the present study may be one of the possible reasons for that.
With regard to retreatment after relapse, little is known about the efficacy, tolerability, or SVR predictors. Recently, Berenguer et al. reported that SVR was achieved in approximately one-third of re-treated patients which could be predicted with the same variables used for naïve LT recipients (19). In the present study, four patients who underwent retreatment after relapse showed RVR or EVR (100.0%), with two achieving SVR (50.0%) and the other two maintaining continuous negative HCV-RNA on third treatment after re-relapse (Fig. 2). Even though the number of patients was small, the result is encouraging. Therefore, we need to be more concerned about aggressive approach of retreatment for relapsed recipients.
The present study had some limitations, including the small number of patients included. We cannot be sure to extend or apply this result to other general cohorts, especially Caucasians or African Americans with respect to IL-28B genotype. More studies and long-term follow-up in this field are needed in the future.
With direct acting antivirals, strategies for HCV recurrence after LT has undergone a startling transformation. With these agents, there is renewed hope of better outcomes for HCV related recipients (568383940). However, in the field of LT, there are some limitations of their use due to safety and tolerance issues. Studies in this field are at an early phase. In many countries including Korea, direct acting antivirals are not approved or commercialized yet. More practically, their extremely high price may be an enormous obstacle. Therefore, even with several limitations, our strategy and the encouraging results can be useful when the newer antiviral agents are not available.
In conclusion, for recipients who show recurrence of HCV-RNA after LT, active therapeutic strategies based on early protocol biopsies within the first year after LT and directed response-guided standard therapy can give rise to encouraging results.



 XML Download
XML Download