

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Iliopsoas abscess (IPA) is a rare disease, especially in neonates. We present a case of neonatal IPA that on the basis of location, symptoms, and ultrasonographic (US) findings, was initially believed to be an inguinal hernia, which is a more common disease in newborns. However, because of an elevated white blood cell count (WBC) and C-reactive protein (CRP), abdominal computed tomography (CT) was performed, which revealed a multi-septated cystic mass extending into the psoas muscle from the lower pole of the left kidney to the femur neck. These findings were consistent with inflammation and abscess, so broad spectrum antibiotics were initiated, and prompt surgical exploration was performed. After opening the retroperitoneal cavity via an inguinal incision, an IPA was diagnosed and surgically drained. Culture of the abscess fluid detected Staphylococcus aureus sensitive to methicillin. To our knowledge, this is the first description of iliopsoas abscess in a Korean neonate. Additionally, we review cases of neonatal IPA reported in the medical literature.
CASE DESCRIPTION
A 20-day-old male infant was referred to our neonatal unit for herniorrhaphy on February 23, 2014. He was born by cesarean section at 38-weeks gestation with a birth weight of 2,530 g. Perinatal history was unremarkable, with no history of premature rupture of membranes, maternal fever, or postnatal hospitalization. On day 18 after birth, his family noticed swelling and mild bluish discoloration of his left thigh. Swelling of the left groin progressed, and the patient was taken to the pediatric department of a Pusan National University Hospital. On ultrasonography (US), the swelling appeared to be a left inguinal hernia, and the patient was referred to our children's hospital for herniorrhaphy.
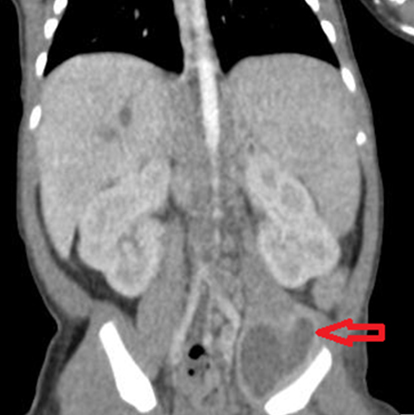
On admission, the infant was afebrile, in good condition, and fed well orally. Physical examination showed swelling of the left groin and medial thigh, but local fever, limited range of motion, paralysis, and abnormal abdominal mass were not noted. Laboratory tests revealed an elevated white blood cell count of 21.33 × 103/mL with 34.0% segmented neutrophils and an elevated CRP of 3.34 mg/dL. Repeat US showed that bowel and echogenic mesentery were herniated into the left femoral area with the distal end of the hernia located in front of the left femur, compressing the left femoral vein medially. A femoral hernia was considered likely, but an abscess or abnormal mass could not be ruled out. Therefore, we performed an abdominal computed tomography (CT), which demonstrated a 2.3 × 1.8 × 3.8 cm septated cystic mass with irregular enhancing thickened wall in the left iliacus muscle, suggestive of a left iliopsoas abscess (IPA) (Fig. 1). Diffuse intra-hepatic duct (IHD) dilatation with mild common bile duct (CBD) dilatation was also present. Ampicillin and cefotaxime were initially administered, and then ampicillin was changed to nafcillin. On hospital day 3, after the retroperitoneal cavity was opened via an inguinal incision, an IPA was diagnosed and surgically drained. A yellowish exudate was aspirated by needle, the abscess cavity was irrigated thoroughly using normal saline, and a Penrose drain was inserted into the abscess cavity. Culture of the abscess fluid was grown methicillin-sensitive Staphylococcus aureus (MSSA), and results of blood, cerebrospinal fluid (CSF), and urine cultures were all negative. Swelling and redness of the leg and inguinal area resolved by the next day. Intravenous antibiotic therapy continued for 3 weeks, and subsequent US examination revealed no residual IPA. Assessment of neutrophil respiratory burst was performed using the dihydrorhodamine flow cytometric assay (DHR test) using flow cytometry, which is used to screen for chronic granulomatous disease, and results were normal. Laboratory evaluation of the patient's IHD dilatation with mild CBD dilatation showed a gamma-glutamyl transpeptidase (GGT) level of 337 IU/L and direct bilirubin of 0.85 mg/dL. The patient was discharged on postoperative day 17 and is doing well at 5 months of age. In the outpatient clinic, a follow-up US demonstrated mild dilatation of the CBD and faint visualization of the intrahepatic portal vein, suggestive of portal vein thrombosis. However, the possibility of septic emboli is unlikely considering that this would be an accidental finding during a month after treatment completion. We will follow up the patient with repeat abdominal US and liver function tests, including GGT, to assess for the diffuse IHD and CBD dilatation over the next few years.
DISCUSSION
Iliopsoas abscess (IPA) is a purulent retroperitoneal collection involving the iliopsoas muscle. It was first described by Mynter (1) in 1881 as "psoitis" and remains a rarely reported condition. In neonates, only 20 cases have been reported to date in English literature (23456789101112131415161718).
Iliopsoas abscesses can be classified as primary or secondary. Primary IPA occurs because of hematogenous or lymphatic spread of a causative organism from a distant site. Secondary IPA occurs as a result of the direct expansion of a nearby inflammatory process into the iliopsoas muscle (19). In neonates, primary IPA is more common, whereas secondary IPA accounts for the majority of cases seen in adults and most often arises from intra-abdominal inflammatory processes, particularly those of intestinal origin (20). With respect to microbiology, the clinical precursor in most cases of neonatal IPA is not detected with only 5reported cases showing a precedent infection; intramuscular hemorrhage (3), umbilical venous catheter infection (5), urethral infection (6), bacteremia (7), and pustular lesion (11). The etiology of our case was also idiopathic, because the patient was a healthy term newborn who had no birth trauma or other perinatal problems.
S. aureus is the most common etiologic agent of IPA, accounting for 18 of 20 reported cases, with 3 cases involving methicillin-resistant S. aureus (2618). Klebsiella pneumonia (7) and Streptococcus pneumonia (4) were reported as pathogens in the other 2 cases. Regarding possible pathogenic mechanism, S. aureus, which is part of the resident flora of the skin and gastrointestinal tract, spreads often hematogenously because of weak immune function in neonates. This provokes an infectious process and inflammation in the iliopsoas muscles, which have an abundant blood supply, and an abscess forms in the psoas region.
The classic triad of pain, fever, and limp that was described by Mynter (1) in 1881 is atypical and is rarely seen. According to the literature, most cases of neonatal IPA present with poor mobility of the lower extremities and femoral swelling; only 3 cases have presented with high fever (>38℃) (2613). In the present case, only swelling and bluish discoloration of the groin and femoral regions developed, whereas poor movement of the leg and high fever were not observed.
Routine laboratory investigations, including complete blood count and CRP are useful for confirming the diagnosis of an inflammatory mass. In many cases of IPA, WBC counts have increased to as high as 20,000-30,000/µL, with this case showing a WBC count of 21,330/µL. Cultures of blood and direct abscess aspirate are the most definitive diagnostic tools available, with the abscess aspirate giving a higher yield and specificity.
IPA is commonly diagnosed via modern imaging techniques, such as US and CT. In spite of its massive radiation dose, CT can estimate the extent and character of a mass more accurately than traditional US. On the basis of the location, symptoms, and US findings in our patient, we initially considered an inguinal hernia, which is a more common disease in newborns, as the most likely diagnosis. Abdominal CT was performed because of the elevated WBC and CRP, leading to surgical exploration during which the IPA was accurately diagnosed and treated. In this respect, CT is the optimal radiographic modality to evaluate for IPA.
Traditionally, treatment of an IPA consists of broad spectrum antibiotics combined with drainage of the abscess through a percutaneous or open technique. Empiric antibiotic therapy should include activity against Staphylococcus aureus (including activity against MRSA in regions where prevalence is substantial) and enteric organisms (both aerobic and anaerobic enteric flora). In previously reported cases (34581112), antibiotic therapy was started before a specimen of the abscess fluid was taken for culture because, as in our case, CRP or WBC count were increased. US-guided percutaneous needle aspiration may be insufficient for drainage of an abscess and prolonged use of antibiotics. Consequently, surgical drainage is indicated if US-guided needle aspiration fails (10).
The prognosis of IPA in neonates is good. All reported patients recovered without any serious problems, such as sepsis, and no abscesses recurred after drainage and antibiotic therapy.
This case has clinical importance due to the rarity of IPAs, the patient was almost sent for a herniorrhaphy. However, timely use of the CT study facilitated a prompt diagnosis, improving the prognosis by accurate management without delay. In conclusion, when a neonate presents with femoral swelling and an elevated CRP level or increased WBC count, IPA must be included in the differential diagnosis.

 XML Download
XML Download