

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Numerous studies and reports have suggested that psychosocial problems increase the risk for mental health problems and increase the need for health care services in children and adolescents (12). Primary care practice is a valuable avenue for treating and/or identifying the need for more specialized behavioral health care including health behavior change, mental health care, management of psychological symptoms and psychosocial distress, and control of substance abuse (2). Frequently, psychosocial problems in children are not treated with early intervention (3). Unfortunately, untreated psychosocial problems in childhood are thought to lead to dysfunctions in adulthood, including conditions that require expensive interventions (4). In the Adverse Childhood Experiences (ACE) study of 17,000 adult patients with medical problems, Van Niel et al. (5) reported that patients with more adverse experience during childhood experienced higher rates of smoking, alcohol abuse, obesity, and physical inactivity. Therefore, early detection and intervention of psychosocial problems in children are important for prevention and amelioration of lifelong ailments and maintenance of community health.
Traditionally, the primary medical service provided by pediatricians has been thought to be an opportunity for recognition of psychosocial problems in children (6). Pediatricians reported that improving training for evaluating and managing behavioral problems in children is necessary to meet the demands of much needed behavioral health care for children and parents (6). However, pediatricians often hesitate to identify psychiatric problems due to lack of psychiatric training (7). In addition, limited time for analysis makes it difficult for primary physicians to detect psychosocial problems in children, especially early in life (8). In fact, the literature has revealed that less than 50% of children are screened by primary care physicians for psychosocial problems, and very few children meet with psychiatrists (7).
For early and effective recognition of psychosocial problems in children, Jellinek et al. (9) designed a screening tool called the Pediatric Symptom Checklist (PSC) in 1986 and then developed it further (9101112). Initially, the PSC was targeted for children 6 to 12 yr old, but was subsequently extended to cover children from 4 to 18 yr of age (913). The PSC has been used successfully in the United States of America (USA) due to its easy application for screening of psychosocial problems. In addition, other countries have adopted the PSC into their own language and culture for screening of psychosocial problems. For example, a Spanish group in the USA studied the reliability and validity of the PSC for children aged 4 to 5 yr (11). Also, children from 7 to 12 yr of age in the Netherlands and 5-yr old children in Austria also were studied for early detection of psychosocial problems using the PSC (1415). However, there is currently few effective tool for screening or early detection of psychosocial problems in Korean children.
Based on the studies conducted in other countries, we hypothesized that a Korean version of the PSC would be a useful tool for early detection of psychosocial problems in children and adolescents in Korea. In the PSC optimized for Korean children, we aimed to suggest cut-off scores for detecting meaningful psychosocial problems.
MATERIALS AND METHODS
Participants
The information for analysis of the PSC was gathered from a clinical sample and a non-clinical sample.
Non-clinical sample
A total of 420 children, ranging in age from 6 to 12 yr, who lived in Daegu, a city in southeastern Korea with approximately 2.5 million habitants, were recruited from local schools. Permission was obtained in advance from the headmaster and teacher and parents' committee of the school board of the school in which the study was performed.
Written protocol and instructions had been distributed to the parents by the delivery of the students in each classroom. Participants were not compensated.
The PSC and the child behavior checklist (CBCL) were distributed to the 420 participants and their parents. A total of 403 students and their parents read the protocol and instructions and returned the PSC and the CBCL (response rate 95.9%). Seventeen participants were excluded due to lack of agreement to participate because of absence having chronic physical illness (n=8), psychiatric problems (n=3) or physical problems (n=6) of students according to teachers' information. After excluding six participants due to even single missing data point in the PSC and the CBCL, the information from 397 children and their parents were used in the analysis.
Clinical sample
One hundred patients who visited the Department of Child and Adolescent Psychiatry, Kyungpook National University Hospital were recruited. Inclusion criteria were 1) age 6-12 yr, 2) diagnosed with a psychiatric disease, 3) no chronic medical illnesses, and 4) living with main caretakers. Among the 100 responses, data from three patients were excluded due to incomplete responses even with a single missing data point. Parents answered the PSC during the waiting time at their first visit. Psychiatric diagnosis of the clinical group made by the child and adolescent psychiatrists had been described in Table 1.
Measure and scales
Pediatric symptom checklist
The PSC consisted of 35 questions regarding the parents' impressions of psychosocial problems in their children (1013). The answer choices consisted of 'never,' 'sometimes' and 'frequently,' which were allocated 0, 1 or 2 points, respectively. Higher PSC scores represented more psychosocial problems in the children and adolescents.
The PSC-Korean version was developed with a forward-backward translation procedure. It was translated by a bilingual person, and a consensus procedure was performed with a Korean child and adolescent psychiatrist. Another bilingual translator performed a blinded backward-translation to English, and the final version of the PSC was obtained after some adjustments. When translating and adapting this instrument, the Korean culture and language were taken into account. Compared to the original version of the PSC, several words and phrases were modified to maintain the meaning. For example, item number 8, 'Daydreams too much' had been translated into 'Dazed often' in Korean because not all Korean people are familiar with the meaning of the word 'daydream'. Item number 29, 'Does not listen to rules' had been translated into 'Disobeys rules' and Item number 34, 'Take things that do not belong to him or her' into 'Steal things' because they were clearer than the directly translated in meaning in Korean. In order to evaluate the test-retest reliability of the Korean PSC, 180 students were randomly selected to complete the PSC scale again four weeks later. Among these 180 participants, 140 returned the second PSC.
Child behavior checklist (CBCL)
The CBCL, developed by Achenbach, is a tool for the assessment of children and adolescents (16). It consists of two parts: a social competence scale and a syndrome and total problem scale. A CBCL-Korean version has already been developed and is currently used by clinicians (17). The CBCL-Korean version consists of a 132-item questionnaire, and responses are provided on a three-point Likert scale from 0 to 2. The social competence scale assesses social interaction, school performance and overall social competence. In school performance scale, average scores of total 5 subjects has been calculated such as Korean, mathematics, social science, science, and English, only in case of middle school students. The syndrome and total problem scale includes social withdrawal, somatic complains, anxiety, depression, attention problems, aggressive behavior, externalized dysfunction, internalized dysfunction and dissocial behavior. Higher CBCL scores represent more severe psychosocial problems. The score is recorded as a raw score and is translated into a T score. Although a 63 or more T score (90 percentile) has been generally considered clinical, the clinical referred cut-off score is a 60 or more T score (85 percentile) in non-clinical samples and a 70 or more T score (98 percentile) in clinical samples. In this study, we used a 60 or more T score, because we developed the PSC to screen psychosocial problems in a general population of children and adolescents.
Statistical analysis
Demographic variables between the non-clinical and clinical groups were analyzed with a t-test and a chi-square-test. The internal reliability and test-retest reliability of the PSC were assessed with Cronbach's alpha and Pearson's correlation coefficient (r). The inter-correlation fit among the four factors in the PSC was assessed using confirmatory factor analysis (CFA) with structural equation modeling (18). For the validity of the PSC-Korean version, transformed CBCL scores (total, internalizing and externalizing scores) were correlated with total score of the PSC-Korean version (Pearson's correlation coefficient, r) as was performed in the development of the PSC-Dutch version (14). One-way ANCOVA was used to demonstrate discriminant validity of the Korean version of the PSC between the non-clinical group and clinical group with the covariates of sex, parental educational status, and economic status. The cut-off score was determined via receiver operating characteristic (ROC) analysis of the CBCL score (total problem score, internalizing score and externalizing score), clinical group scores and non-clinical group scores. All statistical analyses were performed with SPSS 13.0 for Windows and LISREL 8.80.
RESULTS
Demographic data
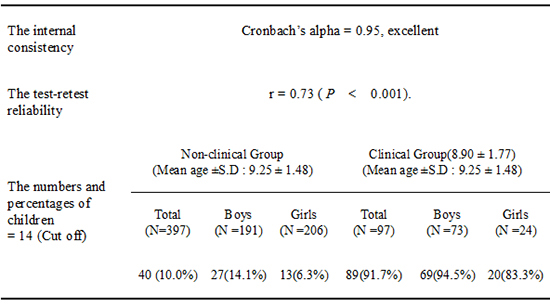
The mean age of all the subjects was 9.3±1.5 yr. The mean age and years of education for the parents who filled out the PSC were 37.3±2.9 and 15.3±1.8, respectively (Table 1). There were no significant differences in age, parent age or parenting status between the non-clinical and clinical groups. The mean age of the non-clinical and clinical groups was 9.25±1.48 yr and 8.90±1.77 yr, respectively. However, there were significant differences in years of parents' education (father: t=5.98, P<0.001, mother: t=6.71, P<0.001) and social economic status (χ2=83.5, P<0.001) between the groups. The mean years of education in the clinical and non-clinical groups were 14.34±1.29 yr and 15.53±1.00 yr, respectively. The clinical group comprised more participants in the lower-middle social economic status compared to the non-clinical group (χ2=83.50, P<0.001) (Table 1).
Pediatric symptom checklist-Korean version
The internal consistency of the PSC-Korean version was excellent (Cronbach's alpha=0.95). The test-retest reliability was r=0.73 (P<0.001). However, a poor model fit was observed in confirmatory factor analysis (CFA) (χ2=1,852.0 at df=554; P<0.001; goodness-of-fit index [GFI]=0.821, adjusted GFI=0.797, root-mean-square error of approximation [RMSEA]=0.069 [90% confidence interval, 0.065-0.072], root-mean-square residual [RMR]=0.015). The mean PSC total scores of the non-clinical and clinical groups were 5.2±6.1 and 27.0±10.1, respectively (F=3.64, P=0.01). The total score of the PSC positively correlated with total CBCL (r=0.85, P<0.01), internalizing score (r=0.73, P<0.01) and externalizing score (r=0.79, P<0.01) (Table 2). Using CBCL scores and experience of the staff at providing psychiatric service, the ROC curve was calculated and is shown in the upper-left corner of Fig. 1. All areas under the ROC curves (AUC) were greater than 0.9 and had statistical significance (Table 3). Using clinical CBCL scores (CBCL total score≥60, CBCL externalizing score≥60, CBCL internalizing score≥60) and presence of clinical diagnosis, the recommended cut-off score of the PSC was 14. Considering the diagnosis made by child and adolescent psychiatrists as the gold standard, the sensitivity and specificity of the PSC-Korean version with a cut-off score of 14 were 91.8% and 89.9%, respectively (Table 4). When using the 28 score cut-off of the USA, 44.3% of the clinical group and 0.5% of the non-clinical group were identified as a risk group with psychosocial problems (13).
DISCUSSION
Using 494 Korean children aged 7-12 yr, the current study assessed the reliability and validity of a Korean version of the PSC and suggested a cut-off for recommending further clinical assessment. The results suggest that the Korean version of the PSC has good internal consistency and validity using the standard of CBCL scores.
The internal consistency of the Korean version of the PSC in the current study was excellent (Cronbach's alpha=0.95). The original version of the PSC has also good internal consistency (Cronbach's alpha=0.91) (10). In addition, the US version (Cronbach's alpha=0.92), the Spanish version (Cronbach's alpha=0.91) and the Dutch version of the PSC (Cronbach's alpha=0.89) also have been reported to have excellent internal consistency (1419). The test-retest reliability correlation in the original version of the PSC was r=0.84 - 0.91, and that of the Korean version was r=0.73 (10). Stoppelbein et al. (20) suggested a test-retest reliability (r=0.77) in patients with chronic diseases which is similar to our results. Anastasi et al. (21) reported that a test-retest reliability correlation value higher than 0.70 could be accepted as reasonable.
Factor analysis of the original PSC has found that the measure loads significantly onto three brief subscales for use in identification of attentional, internalizing (depression/anxiety), and conduct problems including the children's depression inventory (CDI) for depression, the screen for child anxiety related emotional disorder (SCARED) for anxiety, and the ADHD scale of the child behavior checklist for attention problems (9101319). The Korean version of the PSC showed a poor model fit in CFA, as did the Dutch version of the PSC (14). These poor fits may be due to the fact that items on school life had been divided into the factor of internalizing and conduct behaviors. Moreover, different cultural and psychological backgrounds might affect the poor fits compared to those of the original version. However, future studies are needed to verify this conjecture. The correlation between the Korean version of the PSC and the CBCL scores was significant (r≥0.70). These high correlation values suggest that the Korean version of the PSC reveals four latent psychosocial problem dimensions including internalizing, externalizing, attention, and school problems, similar to that proposed by Gardner (18). In ROC curve analysis, AUC values were greater than 0.9. In addition, participants in the clinical group scored significantly higher than those in the non-clinical group. Taken together, these results suggest that the Korean version of the PSC has excellent internal consistency and good reliability and validity.
In a number of validity studies, PSC case classifications agreed with case classifications on the child behavior checklist (CBCL), children's global assessment scale (CGAS) ratings of impairment, and the presence of psychiatric disorder in a variety of pediatric and subspecialty settings representing diverse socioeconomic backgrounds (1019). When compared to the CGAS in both middle and lower income samples, the PSC has shown high rates of overall agreement (79%; 92%), sensitivity (95%; 88%) and specificity (68%; 100%), respectively (9).
When the clinical cut-off of the PSC-Korean version was set at 28, the detection rate of psychological dysfunction in the non-clinical group was less than 1%. However, this high cut-off only detected 71.1% of children in the clinical group. When the cut-off of the PSC-Korean version was set at 14, the detection rate of psychological dysfunction in the non-clinical group was greater than 10%. Indeed, in an epidemiology study of school-aged children, the detection rate of psychosocial dysfunction was in the range of 12% to 20% (2223). Studies using the PSC have found prevalence rates of psychosocial impairment in middle class (~12%) that are quite comparable to national estimates of the prevalence of psychosocial problems (1019). With a cut-off of 14, the detection rate in the clinical group was improved to 91.7% (Table 4). Taken together, these results suggest that the cut-off score for the PSC-Korean version should be 14. Children with psychosocial problems could be also included in the non-clinical group as 40 children (10%) in Table 4. In comparison, the US version of the PSC has a cut-off of 28, the Dutch version has a cut-off of 22 (1314), the Brazilian version has a cut-off of 21, the Japanese version has a cut-off of 17 and the Mexican version has a cut-off score of 12 (1314242526). In the Mexican sample, the PSC has been validated by Mexican-Americans in low-income US communities and the educational level of parents was lower than in our sample (1317).
When comparing the results of behavioral questionnaires between American and Korean children, the scores of other checklists such as the CBCL, the ADHD rating scale, the child sexual behavior inventory (CSBI), the adolescent dissociative experience scale (A-DES), the child report of post-traumatic symptoms (CROPS) and the parent report of post-traumatic symptoms (PROPS) were lower for Korean children (2728293031). Common characteristics of countries with lower scores and lower clinical cut-off recommendations, such as Korea, may be a reflection of real differences in psychological symptoms. However, these scores may also reflect low parental sensitivity to psychological problems (29). Korea is one of the countries in which subjects show a response bias because they want to give an answer that is as socially desirable as possible (28).
There were several limitations in the current research. First, the participant pool was recruited from a small area of Korea, so it may not reflect the entire Korean population. In the clinical group, more males had been recruited and females had been younger in age. Second, the sample could not be screened with a structured clinical interview nor with a clinical global impairment-score. Future studies should consider recruiting from a broad area and including a structured interview and correlation of the scores of subscales of the PSC with the psychiatric diagnosis of patients of child and adolescents. In the clinical group, children with externalizing symptoms such as attention deficit/hyperactivity disorder and oppositional defiant disorder were more prevalent (60.9%) compared to those (25.7%) with internalizing disorder such as major depressive disorder, selective mutism and separation anxiety disorder.
The Korean version of the PSC has a good internal consistency and validity using CBCL scores as a standard. Thus, the Korean version of the PSC may be a useful tool for the early detection of psychosocial problems including behavioral and emotional problems in Korean children.




 XML Download
XML Download