

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Female urethral cancer (UCa) is a rare malignancy; it accounts for approximately 1% of all female urological cancer (1). Initial signs of UCa, such as voiding symptoms and bloody spotting, are ignored in most patients with female UCa because they are not pathognomonic. In fact, voiding symptoms and bloody spotting are common indicators of non-malignant conditions in normal healthy females. Despite improvements in diagnostic imaging, delayed diagnosis remains a challenge in these patients (2). Because initial diagnosis is delayed, female UCa patients often present with large and advanced lesions at initial diagnosis, which results in poor prognosis (3). More importantly, because female UCa is rare, the key prognostic factors remain poorly defined, and optimal therapeutic strategies are primarily based on limited evidence (4).
Given these challenges, all available evidence should be shared and discussed so that the current knowledge base about female UCa is improved. Additionally, previous studies were largely based on Western populations, so more evidence is required to improve our understanding of female UCa in Asian countries. In this study, we evaluated 19 cases of female UCa in Korea and reported useful information about clinical features, treatment, and prognostic factors.
MATERIALS AND METHODS
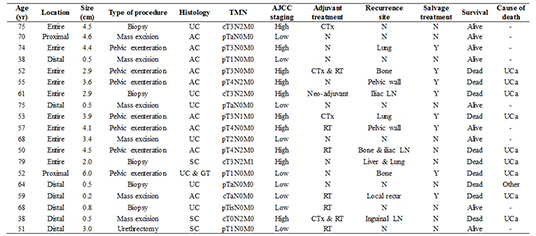
We reviewed medical records of 21 consecutive patients diagnosed with female UCa at our institution between August 1991 and April 2012. After two cases were excluded due to undefined histologic features, we finally examined 19 patients of female UCa. We evaluated the following variables associated with patient characteristics: age, initial presenting symptoms, procedure type, whether or not the patient received adjuvant therapy, histologic type, tumor size and location, recurrence and sites, whether or not the patient received salvage therapy, and recurrence-free (RFS), cancer-specific (CSS) and overall survival (OS). Tumor location was classified as proximal, distal, and whole urethral involvement, as in a previous report (5). Proximal tumors were defined as tumors limited to the proximal two-thirds of the urethra, while tumors were classified as "distal" if they were limited to the distal one-third of the urethra. The surgical modalities at presentation included mass excision, urethrectomy, and pelvic exenteration. Pathological stages were determined according to the 7th edition of the American Joint Committee on Cancer (AJCC) staging system (6). Stage Ta, T1, and T2 tumors with N0 and M0 were defined as low stage tumors, while stage T3 and T4 tumors with N1-2 and M1 were classified as high stage tumors (6). The pathological T stage was primarily used to determine T stage. However, in cases where there was no documentation of pathological T stage, clinical T stage was used. Local recurrence was defined as cancer reappearance at the operative sites or in the pelvic cavity, and distant recurrence was tumor relapse at other sites besides the pelvic cavity.
The Kaplan-Meier method was used to calculate survival outcomes (RFS, CSS, and OS) after initial treatment, and log-rank tests were used to determine statistically significant differences between survival curves. We used a Cox proportional hazards model to identify significant predictors of survival outcomes according to clinicopathological variables. We rejected the 2-sided null hypothesis that there was no significant difference in cases where the P value was less than 0.05. Consistently, we rejected the null hypothesis if the 95% confidence interval (CI) of point estimates excluded 1. All statistical analyses were performed using SPSS software, version 19.0 (IBM Corp., Armonk, NY, USA) and GraphPad Prism (GraphPad Software Inc., La Jolla, CA, USA).
RESULTS
Patient characteristics and overall prognoses are summarized in Table 1. Seven patients were diagnosed by physical examination only, not by imaging studies. The median patient age at the time of diagnosis was 59.0 yr, and the median follow-up duration was 87.0 months. Initial presenting symptoms were varied. Voiding symptoms and blood spotting were the most common and only 1 patients had no symptoms. The median tumor size was 3.4 cm. With regard to tumor staging, 9 patients (47.4%) had low stage tumors and 10 patients (52.6%) had high stage tumors. Additionally, the pathological findings were histologically diverse. Adenocarcinoma was the most common type and urothelial carcinoma was the second most common.
Fig. 1 is a flow chart of the types of primary and adjuvant therapy used to treat patients. While 5 patients underwent biopsies without other surgical procedures, 14 patients underwent surgery including pelvic exenteration, urethrectomy, and local mass excision. For the 7 patients who received adjuvant therapy, such as radiation and systemic chemotherapy, there was no dominantly employed modality. Overall, 57.9% of these patients (n=11) experienced tumor recurrence after primary therapy. The rates of lymph node and bone metastases were the same (27.7%), and these were the most common sites of recurrence. Summarized information for all 19 patients evaluated in this study is also provided in Table 2.
Fig. S1 shows the oncological outcomes (RFS, CSS, and OS) of the patients in this study. The 5-yr RFS, CSS, and OS rates were 34.8% (standard error [SE] 22.7%-46.9%), 58.9% (SE 46.8%-71.0%), and 58.9% (SE 46.8%-71.0%). All oncological outcomes were significantly different between patients with low stage (stage I-II) and high stage cancer (stage III-IV) (Fig. 2). When patients were classified by T stage, patients with advanced T stages (≥T3) had poor survival outcomes for RFS, CSS and OS compared to patients with localized tumors (≤T2) (Fig. 3). Patients with positive lymph nodes also had worse survival outcomes by all measurements compared to node-negative patients (Fig. 4). However, only RFS, but not CSS and OS, was worse in patients with tumors involving the entire urethra compared to patients with proximal or distal tumors (Fig. S2).
To identify predictive factors for oncological outcomes, we used a Cox proportional hazards ratio regression model (Table 3). In this analysis, positive lymph node status and advanced T stage (≥T3) were the significant factors for prediction of all oncological outcomes. Additionally, tumor location (entire urethral involvement) was the significant predictor only for RFS, and not for CSS or OS.
DISCUSSION
In the present study, we examined the clinical experiences of 19 patients with female UCa at a single tertiary institution. Despite the small sample size and retrospective nature of this study, it is important to report all available evidence so that we can improve our understanding of this rare malignancy. Notably, we found that cancer stage based on the AJCC classification, T stage, and lymph node status were associated with remarkable differences in RFS, CSS, and OS between patient groups in Kaplan-Meier analysis. Patients with high stage tumors (stage III-IV), advanced T stage (≥T3), and positive lymph nodes had poor outcomes as indicated by all analyzed survival outcomes (RFS, CSS, and OS) compared to their counterparts. Importantly, lymph node positivity and advanced T stage were significantly predictive for poor outcomes in all survival estimates in Cox regression analysis. Additionally, involvement of the entire urethra remained as a predictor of RFS, but not CSS or OS.
Other studies support our results regarding the key prognostic factors for female UCa. Champ et al. (7) analyzed the female UCa patients in the Surveillance, Epidemiology, and End Results (SEER) database and reported that older age, pathological T stage, lymph node positivity, and non-squamous histology were significantly related to poor CSS. Dimarco et al. (5) suggested that pathological T stage was a strong predictive factor for RFS and CSS. Pathological findings about lymph node status were also shown to predict survival in their study. A single center study by Thyavihally et al. (8) reported that patients with early stage cancer (stage I-II) according to the AJCC staging guidelines for female UCa had better survival outcomes compared to patients with advanced stage tumors (stage III-IV), regardless of the treatment modality.
Although other variables such as tumor size, histologic type, and treatment modality were not associated with any oncological outcomes in the present study, these factors have been reported as significant prognostic factors for female UCa by other studies. Bracken et al. (3) evaluated 81 cases of female UCa and found that patients with large tumors (>4 cm) had a lower 5-yr survival rate (about 13%) compared to patients with small tumors (<2 cm), (about 60%). Proximal tumors and lesions that involve the whole urethra have commonly been shown to be associated with poor oncological outcomes compared to distal lesions (9). Benson et al. (10) reported that all patients with proximal urethral tumors died, while 50% of patients with distal urethral tumors survived. The histologic type of female UCa has also been suggested as a key determinant of prognosis (2711). The predominant tumor types are squamous cell carcinoma and urothelial carcinoma, and localized tumors of these histologic types are associated with better survival outcomes compared to tumors of less common histologic types, such as adenocarcinoma (21213). In a study by Meis et al. (14), most patients with adenocarcinoma had locally advanced disease involving adjacent tissues or lymph node metastasis, and approximately 60% of these patients experienced cancer-related death within 2 yr of diagnosis. In contrast to these findings, Dalbagni et al. (1) examined 72 females with primary UCa and reported that primary stage, lymph node status, and tumor site were key independent predictors of survival, but histologic type was not. Dimarco et al. (5) also found that tumor histology was not a significant predictor of recurrence or survival for female UCa patients. They noted that pathological stage was the most important factor for prediction of prognosis. In our analysis, nearly half of the patients (n=9; 42.9%) were diagnosed with adenocarcinoma at the time of presentation; these patients tended to have poor oncological outcomes, though the results were not statistically significant (data not shown).
As discussed in previous studies, therapeutic policies are typically determined by tumor size, location, and aggressiveness (4). For example, surgical resection or radiation can be applied to small (<2 cm) distal lesions, while a combination of radical surgery and radiation therapy is recommended for more advanced stage disease (1516). Our results consistently demonstrated that patients who underwent aggressive surgery and received adjuvant radiation had mainly larger tumors (≥3-4 cm) and tumors that involved the entire urethra. Although multimodal treatment with surgery, radiation, and systemic chemotherapy could be beneficial for selected patients with advanced stage cancer, the role of adjuvant chemotherapy has not yet been definitively shown to improve oncological outcomes (25). In the present study, 2 patients with advanced stage lesions received chemoradiotherapy. Despite the use of combination therapy, these patients experienced tumor recurrence to the bone and inguinal lymph node, respectively, and eventually died as a result of their UCa.
We should consider the limitations of our study. First, the data were collected and reviewed retrospectively. Second, 5 urologic surgeons managed female UCa patients at our institution during the long study period. Therefore, there was some difference in the treatment and follow-up protocols for the patients with this rare malignancy. Finally, although this is the largest report of female UCa in Korea, the statistical power of this study was limited by insufficient number of cases.
In conclusion, high stage, advanced T stage, and lymph node positivity are associated with poor prognosis for all analyzed survival outcomes (RFS, CSS, and OS) in female UCa patients after primary treatment. Furthermore, lymph node status and T stage are significantly predictive of all survival outcomes. Therefore, early diagnosis and management with early identification of this rare malignancy can improve the overall prognosis of UCa patients. Despite the limited case number, our results provide valuable information that expands the current knowledge about clinicopathological characteristics and factors that predict long-term prognosis of UCa patients.






 XML Download
XML Download