

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Eosinophilic gastroenteritis (EGE) is an uncommon inflammatory disorder of the gastrointestinal (GI) tract of unknown etiology. Recently, allergic mechanisms have been implicated in a subset of patients (1). The recently accepted diagnostic criteria for EGE were suggested by Klein et al. in 1970 (2) and revised by Talley et al. in 1990 (3). Criteria include the presence of recurrent GI symptoms, demonstration of a dense eosinophilic infiltration in the GI tract or a high eosinophil content in ascites, and the absence of parasitic or extraintestinal diseases that could cause eosinophilia such as neoplasms, drug reactions, or vasculitis. Peripheral eosinophilia is currently not essential for the diagnosis of EGE (4).
In some cases, histological specimens are difficult to obtain, and as a result there are many instances of misdiagnosis or missed diagnosis of EGE in clinical practice (5). Epidemiological features and the natural history of EGE have not been fully delineated, and treatment options are based mainly on empirical experience.
This study aimed to evaluate the clinical characteristics of mucosal type eosinophilic gastroenteritis (endoscopic, histological features, and response to therapy). We also studied the differences between the infant and child groups and between the histologic EGE (hEGE) and possible EGE (pEGE) groups.
MATERIALS AND METHODS
Study subjects
Thirteen patients in the hEGE group and 9 patients in the pEGE group were enrolled in this study. A retrospective cohort study was performed to assess the differences in clinical characteristics, endoscopic and histological features, and therapeutic effects between the hEGE and pEGE groups. All cases were diagnosed at the Department of Pediatrics in Kyungpook National University Hospital from January 2005 to January 2013.
The following criteria were needed for diagnosis in the hEGE group: 1) GI symptoms present, 2) eosinophilic infiltration of the gastric mucosa with ≥ 10 eosinophils or duodenal mucosa with ≥ 20 eosinophils per high-power field on microscopic examination, 3) no evidence of eosinophilic involvement of organs outside the GI tract, and 4) no evidence of other potential causes of eosinophilia. The pEGE group included patients who met all the criteria except for the second criteria, but had clinical characteristics and a course consistent with a diagnosis of EGE. Patients with the muscular or serosal type of EGE, parasitic infection, vasculitis, and other causes of acute gastroenteritis (infection, drug) were excluded. The hEGE group was divided into infant (age <1 yr-old) and child (age ≥1 yr-old) groups based on age, and the differences between these two groups were investigated. Suspected allergens were evaluated based on the history of allergic response after repeated exposure to suspected foods.
Laboratory tests
Complete blood cell count (including white blood cell count, eosinophil count), C-reactive protein (CRP) levels, erythrocyte sedimentation rate (ESR), serum total immunoglobulin-E (IgE) levels, and specific IgE tests by either immunoCAP (CAP system, Pharmacia-Upjohn, Uppsala, Sweden) for milk, egg, soy, wheat, pork, and cod fish, or the multiple allergen simultaneous test (MAST, AdvanSure Alloscan, LG Life Sciences, Daejeon, Korea) for 41 food allergens were carried out. Serum total eosinophil count >450/µL or >5% of leukocytes was considered as eosinophilia and a specific IgE value >0.35 kIU/L was considered positive. MAST results were interpreted as class 0-6 and class ≥3 was considered as positive.
Endoscopic and histologic evaluation
Esophagogastroduodenoscopy was performed in all enrolled subjects, and gastric mucosal specimens were obtained. Duodenal biopsy was performed in 7 cases in the hEGE group (2 cases in the infant group and 5 cases in the child group) and in 6 cases of the pEGE group. Specimens were obtained from the gastric and duodenal mucosa and the slides were reviewed by experienced gastrointestinal histopathologists. Eosinophil count was analyzed in gastric and duodenal biopsy specimens in 10 high power fields (HPF).
Statistics
For statistical analysis, variables are represented by percentages. The independent t-test was used to compare continuous data and the chi-square test was used for categorical data. P<0.05 was considered significant and statistical analysis was performed using SPSS V.18.0 (IBM, New York, USA).
RESULTS
Subject characteristics
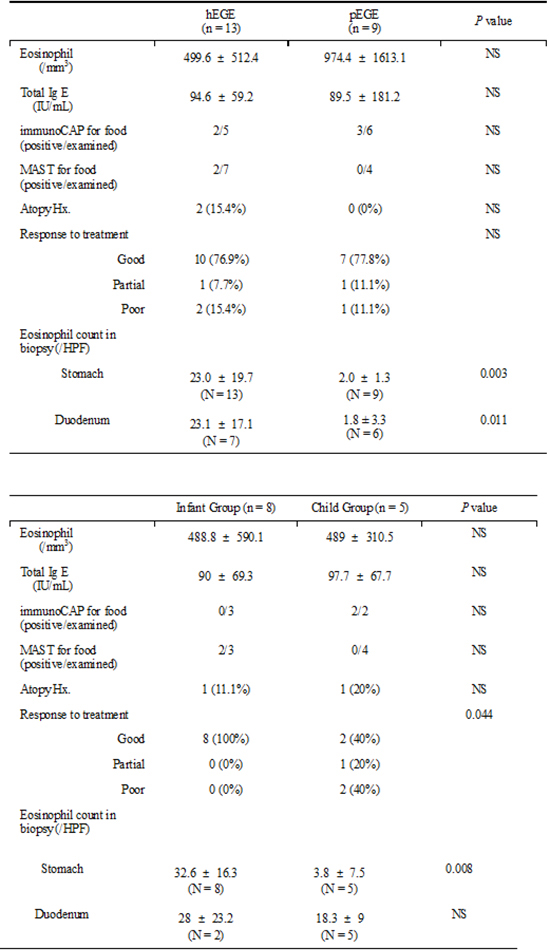
The hEGE group consisted of 13 patients (6 boys, 7 girls) with a mean age of 2.8 yr (range, 0-12 yr). The pEGE group was composed of 9 patients (3 boys, 6 girls) with a mean age of 4.3 yr (range, 0-13 yr). There were no specific differences between the hEGE group and the pEGE group in laboratory study results and clinical characteristics except for biopsy eosinophil counts (Table 1). In the hEGE group, eight patients (61.54%) were categorized in the infant group and 5 patients (36%) were categorized in the child group. A comparison of the infant and child group characteristics is shown in Table 2.
Clinical manifestation
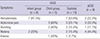
In the hEGE group, initial symptoms included hematemesis (53.8%), recurrent abdominal pain (23.1%), recurrent vomiting (15.4%), melena (15.4%), and edema of the lower extremities (7.1%). Hematemesis was the most common symptom in the infant group (7 patients, 87.5%) and recurrent abdominal pain was the most common symptom in the child group (3 patients, 60%) (Table 3). Suspected allergens based on the patient history were cow's milk (76.9%), egg white (15.4%), crab (7.7%), and peach (7.7%) (Table 1).
Laboratory studies (Table 1)
In the hEGE group, serum total eosinophil counts were elevated in 2 cases (15.4%). Mild elevation of serum total IgE level was found in 2 patients (15.4%). Specific IgE testing was performed in 5 patients and was positive in 2 patients. One patient was positive for cow's milk (0.5) and egg white (0.76), and the other patient was positive for egg white (1.0) in the immunoCAP test.
In the pEGE group, serum total eosinophil counts were elevated in 5 cases (55.6%). Elevation of serum total IgE level was found in 1 patient (11.1%). Specific IgE was performed in 6 patients and was positive in 3 patients (50%). Two patients (33.3%) were positive for cow's milk (7.42, 1.0) and one patient (16.7%) was positive for egg white (0.73) in the immunoCAP test.
Endoscopic and histologic findings (Table 4)
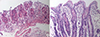
In the hEGE group, 3 subjects (21%) showed normal endoscopic findings, 2 cases (14%) showed mild mucosal edema or erosion (Fig. 1), and 1 case (7%) showed linear hemorrhage and easy friability of the gastric mucosa (Fig. 2). Eosinophilic infiltration was found in gastric mucosa of all 8 patients (100%, Fig. 3A). Eosinophil counts in the gastric mucosal biopsy were 23.0±19.7 in the hEGE group and 2.0±1.3 in the pEGE group (P=0.003). Eosinophil counts in the duodenal mucosal biopsy were 23.1±17.1 in the hEGE group and 1.8±3.3 in the pEGE group (P=0.011) (Table 1).
In the child group, duodenal eosinophilic infiltrations were found in 5 patients (100%, Fig. 3B). The infant group showed a higher eosinophil count than the child group in the gastric mucosal biopsies (32.0±16.3 vs. 3.8±7.5, P=0.008) (Table 2).
In the pEGE group, 1 patient showed mildly hyperemic mucosa (11.1%), 1 patient showed multiple yellowish discoid spots in the duodenum (11.1%), and 7 subjects showed mild mucosal erosion (77.8%).
Treatment and therapeutic effect (Table 5)
Eight patients in the hEGE infant group showed clinical improvement after switching from cow's milk feedings to special formula (extensively hydrolyzed formula or amino acid formula) or breast milk feedings with cow's milk restriction in the mother. One patient in the child group had protein-losing enteropathy and was treated with intravenous solumedrol and oral corticosteroid medications along with milk avoidance. This patient's hypoalbuminemia improved with therapy. Three patients gradually improved with ketotifen treatment and food restriction. One patient with recurrent symptoms required treatment with an oral corticosteroid medication. Response to treatment was better in the infant group (P=0.044).
In the pEGE group, 5 patients showed clinical improvement after switching from cow's milk feedings to special formula or breast milk feedings with cow's milk restriction in mother. Two patients gradually improved with ketotifen treatment and food restriction. One patient with intermittent symptoms required treatment with an oral corticosteroid medication.
DISCUSSION
EGE is a rare disease of unknown etiology characterized by eosinophilic inflammation of the GI tract, affecting children as well as adults (6). Kaijser (2) first described this disorder in 1937. In 1970 Klein et al. (3) defined three patterns of this disease, predominantly mucosal disease, predominantly muscular disease, and predominantly subserosal disease, based on the clinical manifestations. Patients have a varied clinical presentation depending on the anatomical location of the eosinophilic infiltrates and the depth of GI involvement. The mucosal form is the most common and is characterized by nausea, vomiting, abdominal pain, diarrhea, bloody stools, and protein-losing enteropathy. The muscularis form may present with obstructive GI symptoms due to GI wall thickening (7). The serosal form presents with ascites or peritonitis and is least common. This form shows higher peripheral eosinophil counts than the other forms (38). Classification based on histopathological findings is sometimes difficult because of eosinophilic infiltration within the multilayer or inappropriate biopsy. Patients with the mucosal form of EGE (22 cases) were included in our study.
The etiology and pathogenesis of EGE are not well understood. Eosinophils play an important role in the mechanism of tissue injury and it appears that EGE may result from the interaction of a genetic predisposition with food allergy (910). Several epidemiological and clinical features suggest an allergic component (1112). Since some patients improve with allergen avoidance or diets designed to eliminate allergens, food allergy is considered as one possible cause (6). However, anaphylactic reactions to food occur only in a minority of patients. Recently, cell-mediated hypersensitivity has been implicated, and this may provide an explanation for the patients with negative results of allergen-specific IgE testing. Therefore, EGE is considered to be a combination of IgE-mediated food allergy and cell-mediated hypersensitivity (13).
Aquino et al. (14) reported two cases of EGE in monozygotic twins, indicating a genetic basis for the disease. Tien reported that 71.4% of pediatric patients had peripheral eosinophilia and 66.7% had elevated serum IgE levels (15). In comparison, our study showed a lower incidence of eosinophilia, elevated IgE levels, or allergic factors than the previous reports; 14% (2 cases) of patients had peripheral eosinophilia, 14% (2 cases) of patients had elevated serum IgE levels, 14% (2 cases) of patients had allergy to certain foods, and only one patient (7%) had a history of atopy. We suspect that these results may be because we had a higher proportion of infants, in whom allergic diseases may not have yet been fully expressed.
The diagnosis of EGE was made by the presence of GI symptoms, eosinophilic infiltration of the GI tract, typical radiological findings, peripheral eosinophilia, and the absence of parasitic or extra-intestinal disease (68). Testing for parasites was not done on all patients, and this may be a limitation of this study. However, the patients were very unlikely to have had a parasitic infection because most of them improved without specific treatment for a parasitic condition.
Since the clinical presentation is nonspecific, and there is no specific laboratory test, the diagnosis of EGE is based on histology (1617). Eosinophilic infiltration was not always found in sites that appeared abnormal on endoscopy or radiography, and conversely eosinophilia was found in areas with a relatively normal appearing mucosa (1819). In our study, three of the subjects (23.1%) showed normal endoscopic findings. Therefore, if EGE is suspected, multiple biopsies of both the abnormal and relatively normal appearing mucosa should be obtained if possible. Multiple biopsies were not taken in this study due to ethical issues, and this may be another limitation of this study.
The treatment of EGE is empirical. Many reports suggest symptomatic treatment, allergen-elimination, corticosteroids, anti-allergy medications, or immunomodulatory therapies (202122). If specific food allergens are suspected or confirmed, dietary therapy should be considered. Corticosteroids are an effective therapy in children who do not respond to dietary therapy. Steroids improve the clinicopathologic features after several days or weeks of treatment, but sometimes improvement takes several months (2324). Although allergen-elimination and early corticosteroid treatment lead to the improvement of clinical symptoms in the majority of cases, long-term medical treatment and follow-up are required to prevent a relapse. Other potential agents for patients unresponsive to steroids are cromolyn, H1-antihistamines, leukotriene antagonists, or omalizumab. However, the clinical response is variable. In our study, we found most of the patients achieved rapid clinical improvement. In particular, all of the infants improved with switching to breast-feeding, extensively hydrolyzed formulas, or amino acid formula. In the child group, 2 out of 5 patients required corticosteroids in addition to dietary therapy. Possible EGE patients also showed a similarly good clinical course; 7 patients showed clinical improvement with only dietary therapy and one patient improved gradually with ketotifen therapy and food restriction without the need for corticosteroid therapy.
EGE affects all races and any age group from infants to the elderly, but studies in pediatric patients, especially infants, are rare because of its low incidence (152526). There have been few studies on the clinical features of the mucosal type of EGE in infants. In one case report, a one-day-old infant with bloody stools was diagnosed with EGE. He showed milk protein allergy and peripheral blood eosinophilia. His symptoms improved in one week with supportive care and amino acid formula feedings (27). In another report, an 8-month-old infant with vomiting and poor weight gain was diagnosed with EGE. She showed marginally elevated levels of milk-specific IgE and no peripheral eosinophilia. After several months of an elemental diet she gained weight (28). Our study included 8 infants and compared their clinical manifestations and treatment outcomes with those of children with EGE. Infants with EGE predominantly showed the clinical symptom of hematemesis or melena. The clinical outcome in the infant group seemed to be better than that in the child group. In the infant group, duodenal biopsy was performed in only 2 out of the 8 cases due to ethical issues in newborn infants; therefore, there was a limitation in comparing the incidence of eosinophilic infiltration among the different involved sites. Although there are a few case reports of EGE in Korean children (2930), this may be the first retrospective cohort clinical study for EGE in Korean children.
In conclusion, the prevalence of EGE in Korean children has been thought to be very low among pediatric gastroenterologists, but pediatric EGE, including infants, may be more common than previously recognized. Compared with children, EGE in infants seems to have a better clinical course. Because early diagnosis and treatment of EGE is important for prognosis, EGE should be considered in patients with unexplained GI symptoms, even if they do not have peripheral eosinophilia, elevated IgE levels, or abnormal endoscopic findings. The pEGE group in this study was similar to the hEGE group with regard to clinical course and response to treatment. A high index of suspicion is needed for the early diagnosis and optimal management of EGE to minimize the need for a more invasive diagnostic approach.





 XML Download
XML Download