

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Aspergillus spp. became the most common pathogen causing invasive fungal disease (IFD) in immunocompromised patients after the introduction of fluconazole prophylaxis; therefore, invasive aspergillosis (IA) is the most common type of IFD in these patients (123). Immunocompromised patients with IA have a high mortality of 40%-50% (456), and mortality up to 70% has been reported in pediatric cancer patients with IA (7). In spite of the introduction of newer antifungal agents, such as voriconazole and echinocandins, which have an improved effect on IA, the mortality of IA was recently reported as 25%-35% (891011). A relatively higher mortality of 40%-50% due to IA is still cited in situations where amphotericin B deoxycholate was administered as the first line antifungal agent, as in Korea where availability of first line antifungal agents was limited to amphotericin B deoxycholate or itraconazole under government regulations of the national health insurance system (121314).
Given the high mortality of IA and improved prognosis with an early diagnosis and antifungal treatment (1516), empirical or pre-emptive antifungal therapy with antifungal agents having an anti-mold effect has been recommended in immunocompromised patients with risk factors for IA (1718). On the other hand, universal empirical therapy in patients at risk for IA may expose those patients without a true fungal infection to unnecessary antifungal agents, and this may result in unwanted adverse effects and increased medical costs. Actually, only 8%-20% of patients with hematologic/oncologic diseases who received empirical antifungal therapy were reported to have true IFD (192021).
In Korea where empirical antifungal therapy has been standard practice for children with hematologic/oncologic diseases, epidemiological data on IFD or IA in those children is scarce (12). The aim of this retrospective study was to investigate the clinical features and prognosis of invasive pulmonary aspergillosis (IPA) in Korean children with hematologic/oncologic diseases. This study was conducted with consideration of the fact that IA is the most frequent of IFD in immunocompromised patients and most cases of IA are IPA (31112152223).
MATERIALS AND METHODS
Subjects and study design
Medical records of children (<20 yr of age) with hematologic/oncologic diseases, who were admitted to Seoul St. Mary's Hospital, Seoul, Korea between April 2009 and March 2013 were retrospectively reviewed. Among them, children who received antifungal therapy with agents having an anti-mold effect for more than 48 hr were enrolled. The enrolled children were diagnosed with possible, probable, or proven IPA based on the revised definition of IFD in immunocompromised patients recommended by the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC-MSG) Consensus Group in 2008 (24). Children with IA not involving the lung were excluded. Children diagnosed with proven and probable IPA were included in the IPA group, whereas children diagnosed with possible IPA and those who did not fulfill the diagnostic criteria for three categories of IPA were included in the non-IPA group. In the event that one child experienced several episodes of IPA, IPA diagnosed after the cessation of antifungal therapy for a previous episode of IPA was considered a separate episode of IPA and included in the present study. Clinical features of the IPA group were investigated, and clinical factors related to the development of IPA were evaluated by comparing clinical features of the IPA and non-IPA groups. The evaluated clinical features included sex, age, the type of underlying hematologic/oncologic disease and its remission status, the type of therapy administered prior to antifungal therapy, the duration of fever and neutropenia, previous histories of IPA and hematopoietic cell transplantation (HCT), and the presence of concurrent infections. In addition, mortality at 6 and 12 weeks after antifungal therapy was compared between the IPA and non-IPA groups.
Institutional strategies for antifungal therapy
In our hospital, antifungal prophylaxis and empirical antifungal therapy have been given based on the recommendations of the committee for "Guidelines for the Empirical Therapy of Neutropenic Fever Patients based on Literature in Korea" (25). Antifungal prophylaxis with oral fluconazole (3 to 5 mg/kg/day) was given from the initiation of anti-cancer chemotherapy until recovery from neutropenia. In children who received HCT, intravenous micafungin (1 mg/kg/day) prophylaxis was given from the start of pre-HCT conditioning therapy to engraftment, and then oral fluconazole was given until the discontinuation of immune suppressants. Empirical antifungal therapy was administered when fever lasted for 3 to 5 days in children who were expected to have neutropenia for longer than seven days or who received immune suppressants after allogeneic HCT. If chest computed tomography (CT) findings consistent with fungal pneumonia or positive serum galactomannan index (GMI) were observed, pre-emptive antifungal therapy was given regardless of the duration of fever. Serum GMI was tested once or twice a week during neutropenia in children receiving anti-cancer chemotherapy and from pre-HCT conditioning therapy until discharge from hospital in children receiving HCT. Chest CT was performed in children with abnormal findings on chest x-ray or positive serum GMI.
Definition
The diagnosis of IPA was based on the definition of IFD recommended by the EORTC-MSG Consensus Group, which was applicable to patients with host factors of compromised immunity (24). Proven IPA was defined as when Aspergillus spp. were observed with accompanying tissue damage or Aspergillus spp. were identified in culture on sterile materials (24). Probable IPA was defined as when clinical features and mycological evidence for IPA were observed in patients with host factors, and possible IPA was defined as the presence of clinical features of IPA without mycological evidence (24). One of the chest CT findings among well-circumscribed lesions with or without halo sign (consolidation and surrounding ground glass opacity), air-crescent sign and cavity fulfills clinical criteria for IPA, and mycological criteria consisted of the presence of mold or identification of Aspergillus spp. from culture of sputum, bronchoalveolar lavage (BAL) fluid or bronchial brush and positive GMI from serum, plasma or BAL fluid (24). Neutropenia was defined as a neutrophil count <500/µL (24), and chest CT was reviewed by two independent radiologists (HYL and SAI). The GMI was measured using the PLATELIA™ ASPERGILLUS EIA kit (Bio-Rad, Marnes-la-Cocquette, France) in accordance with the manufacturer's recommendations. Serum GMI >0.5 and BAL fluid GMI >1.0 were defined as positive based on the 4th European Conference on Infections in Leukemia (ECIL-4) guidelines (17). Positive GMI results were confirmed by a repeat measurement of GMI in the same sample. Because it was difficult to clearly define whether immunocompromised patients with IPA died of IPA or other complicated causes (26), overall mortality at 6 and 12 weeks after antifungal therapy were evaluated.
Statistical analysis
Categorical variables were compared using the chi-square test and continuous variables were compared using student's t-test or the Mann-Whitney test based on the distribution of the data. Fischer's exact test was used to compare the incidence of IPA during the study period. Mortality at 12 weeks after antifungal therapy was compared between the IPA and non-IPA groups using a log-rank test. Statistical analysis was performed using SPSS Statistics 17.0 (SPSS Inc., Chicago, IL, USA), and statistical significance was defined as a two-tailed P value<0.05.
RESULTS
A total of 268 courses of antifungal therapy with anti-mold agents were administered to 168 children. Among them, one episode of probable cerebral IA and two cases of possible fungal sinusitis without involvement of the lung were excluded. Among the remaining 265 courses of antifungal therapy, 52 (19.6%) episodes of possible IPA, 35 (13.2%) episodes of probable IPA, and two (0.8%) episodes of proven IPA were diagnosed. Accordingly, 37 (14.0%) and 228 (86.0%) episodes were included in the IPA and non-IPA groups, respectively. Candidemia was diagnosed in five (1.9%) episodes in the non-IPA group, and IFD caused by other fungi was not reported. The yearly distribution of IPA was not significantly different during the study period (Fig. 1, P= 0.603).
Characteristics of children with invasive pulmonary aspergillosis
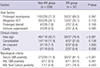
The mean age of children in the IPA group was 11.4±5.3 yr, and 23 (62.2%) episodes of IPA were diagnosed in boys (Table 1). Acute myeloid leukemia (AML) and acute lymphoblastic leukemia (ALL) were the most common underlying diseases, and 23 (74.2%) episodes were diagnosed in non-complete remission (CR) of the underlying hematologic malignancies. In accordance with these results, re-induction or salvage chemotherapy was the most common therapy preceding antifungal therapy (35.1%), and allogeneic HCT was the next most common (16.2%).
Prolonged neutropenia lasting for longer than 10 days was most frequent among the host factors for defining IFD recommended by the EORTC-MSG Consensus Group (Table 2). A halo sign was the most common finding on chest CT, and serum GMI was positive in 30 (81.1%) episodes. BAL fluid analyses were performed in 11 episodes, and BAL fluid GMI was positive in six (54.5%) episodes. Both serum and BAL fluid GMIs were positive in one (2.7%) episode. In the five episodes of BAL cases, BAL fluid GMI were negative, despite of positive serum GMIs. According to GMI results by specimen, BAL fluid(+)/serum(-) group and BAL fluid(-)/serum(+) group showed no significant differences in host factors or in clinical presentation. Bronchoscopy was performed earlier after starting antifungal therapy in the BAL fluid(+)/serum(-) group than in the BAL fluid(-)/serum(+) group, although statistically insignificant (median 3 days, interquartile range [IQR]: 1-12 vs. median 6 days, IQR: 1-11 days, P= 0.173). Aspergillus spp. were identified in BAL fluid cultures in two episodes. Two children diagnosed with proven IPA underwent a pulmonary lobectomy, and the Aspergillus spp. were identified in their excised lung tissue.
Antifungal prophylaxis was performed in 26 (70.3%) episodes, and fluconazole (5 to 10 mg/kg/day) was administered most frequently (Table 3). Amphotericin B deoxycholate was administered as the first line antifungal agent in 33 (89.2%) episodes. The first line antifungal agent was changed to a second line drug in 35 (94.6%) of 37 episodes a median of 4 days (IQR: 2-7) later. Among 33 episodes in which amphotericin B deoxycholate was administered as the first line antifungal agent, amphotericin B deoxycholate was changed to a second line antifungal agent in 32 (97.0%) episodes. Oral voriconazole was given as a second line agent on discharge from the hospital in three (9.4%) episodes, and intravenous voriconazole was given with a diagnosis of probable IPA in four (12.5%) episodes. In six (18.8%) episodes, second line agents were administered due to sustained fever lasting for more than five days in spite of first line antifungal therapy. In the remaining 22 (68.8%) episodes, second line antifungal agents were given due to adverse effects of first line agents. Infusion-related adverse effects of amphotericin B deoxycholate were reported in 18 (56.3%) episodes, including 14 cases of chills, seven cases of high fever, five cases of nausea and vomiting, and one case each of dyspnea, skin rash and severe irritability. Hypokalemia (serum potassium level <3.0 mEq/L) developed in 15 (46.9%) episodes during amphotericin B deoxycholate therapy in spite of potassium supplementation. Increased serum creatinine greater than two times the baseline was observed in three (9.4%) episodes. Finally, antifungal therapy was completed with voriconazole in 27 (73.0%) episodes.
Mortality at 6 and 12 weeks after antifungal therapy was 16.2% and 27.0%, respectively (Table 3). Between 10 children who died within 12 weeks after antifungal therapy and 27 children who survived longer than 12 weeks after antifungal therapy, there were no significant differences in the distribution of host factors and clinical and mycological criteria (data not shown). Voriconazole was administered to 77.8% of the children who survived and 60.0% of the children who did not survive (P=0.407). Voriconazole therapy was begun a median of 7 days (IQR: 4-13) after antifungal therapy in the children who survived and a median of 14 days (IQR: 6-25) after antifungal therapy in the children who did not survive (P=0.204).
Comparison between the IPA and non-IPA groups
Clinical features between the IPA and non-IPA groups were compared in order to identify any significant factors related to the development of IPA in children who received antifungal therapy (Table 1). There were no significant differences in sex, age, underlying disease and its remission status, previous histories of IPA and HCT, and the type therapy administered prior to antifungal therapy between the two groups. However, significantly more children in the IPA group experienced neutropenia lasting for longer than 2 weeks before antifungal therapy (P< 0.001), and accordingly the proportion of children with a total duration of neutropenia longer than 4 weeks was significantly higher in the IPA group compared to the non-IPA group (P< 0.001). Although fever duration was significantly longer in the IPA group than in the non-IPA group, the difference was only one day.
There was no difference in the distribution of host factors for defining IFD recommended by the EORTC-MSG Consensus Group between the two groups (Table 2). Chest CT was performed in 118 episodes in the non-IPA group, and halo signs were observed significantly more frequently in the IPA group than in the non-IPA group (P<0.001). BAL fluid analyses were performed in 28 episodes (11 in the IPA group and 17 in the non-IPA group) between April 2009 and March 2011. In the 17 episodes in the non-IPA group, there were no cases of positive BAL fluid GMI and only one (5.9%) episode of positive BAL fluid culture for Aspergillus spp.
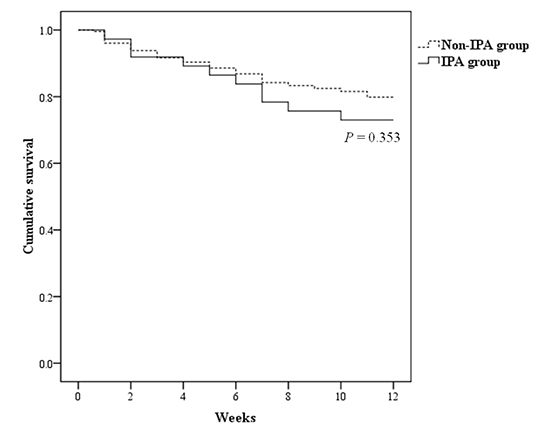
Antifungal prophylaxis was administered more frequently in the IPA group; however, the difference was not significant (Table 3). The type of first line antifungal agent was not significantly different between the two groups. However, second line and later administered antifungal agents were significantly different between the two groups - voriconazole and liposomal amphotericin B were most commonly administered in the IPA and non-IPA groups, respectively. Mortality at 6 and 12 weeks after antifungal therapy was higher in the IPA group compared to the non-IPA group, however, the differences were not statistically significant (Fig. 2, P=0.353).
DISCUSSION
In the present study, clinical features and prognosis of IPA diagnosed in children with hematologic/oncologic diseases were investigated, and clinical factors associated with the development of IPA in children who received antifungal therapy were evaluated. Prolonged neutropenia, corticosteroids or immune suppressant therapy, hematologic malignancy as a underlying disease, especially AML, relapsed leukemia, receiving an allogeneic HCT, graft-versus-host disease and cytomegalovirus infection after allogeneic HCT, and other respiratory viral infection after allogeneic HCT were reported as risk factors for IA in patients with hematologic/oncologic diseases (56827282930). In accordance with previous reports, AML was the most frequent underlying disease, and more than half of the children with hematologic malignancies were non-CR status in the present study.
IPA was diagnosed in 14.0% of children who received antifungal therapy in the present study, and the remaining children, over 80.0%, may have experienced adverse effects of the administered antifungal agents, increased medical costs, and prolonged duration of hospitalization due to unnecessary antifungal therapy. We tried to identify clinical factors predicting the development of IPA in those children to reduce unnecessary antifungal therapy in future patients, and only the duration of neutropenia was significantly different between the IPA and non-IPA groups. Because prophylactic fluconazole has been administered to children at risk for IFD in our hospital, we decided to begin empirical or pre-emptive antifungal therapy based on the risk for IA. As a result, antifungal therapy was initiated based on similar clinical criteria for children both in the IPA and non-IPA groups. Other hospitals where antifungal prophylaxis is performed should address such situations in a fashion similar to our hospital. Therefore, the initiation of antifungal therapy should be based not only on clinical features, but also on results of imaging and mycological tests, such as chest CT and serum and BAL fluid GMIs. In the present study, the incidence of halo sign on chest CT was significantly higher in the IPA group compared to the non-IPA group. Although there was no significant difference in outcome between the IPA and non-IPA groups, chest CT was helpful in diagnosing IPA.
Serum GMI is valuable in diagnosing IPA in children and adults (313233), and the ECIL-4 guidelines recommend a serum GMI >0.5 as positive (17). Considering 16.2% of the IPA group in the present study showed negative serum GMI results but positive BAL fluid GMI or culture results, BAL fluid analyses should be encouraged in patients in whom IPA is suspected in spite of negative serum GMI results. In addition, bronchoscopy should be performed in the early phase of IPA to acquire reliable BAL fluid GMI results. The ECIL-4 guidelines recommend a BAL fluid GMI >1.0 as positive (17). However, there have been only a few studies on the application of BAL fluid GMI for diagnosing IPA in children (3435), and further studies to determine an appropriate BAL fluid GMI cut-off value for diagnosing IPA should be performed in children.
The 27.0% mortality in the IPA group was lower than recently reported 45< mortality in Korean adult and pediatric patients with IPA (1213), although 89.2% of the IPA group received amphotericin B deoxycholate as a first line antifungal agent in the present study. The difference in mortality was assumed to be a result of early changes in antifungal agents from amphotericin B deoxycholate to liposomal amphotericin B or voriconazole in our cases. In addition, about 80% of the IPA group showed halo signs on chest CT, which have been reported as characteristic CT findings in the early phase of IPA as opposed to air-crescent, cavity, and simple consolidation (3136). Most patients in the IPA group may have been diagnosed with IPA in the early phase of disease in the present study, and an improved prognosis in IPA patients with halo signs compared to other CT findings has been reported (37).
The present study was performed when amphotericin B deoxycholate or itraconazole were required to be administered as a first line antifungal agent due to government regulation of the national health insurance system in Korea. Now, in 2015, we are able to administer liposomal amphotericin B and caspofungin as first line antifungal agents in febrile neutropenic children based on a modified government policy in 2014. Because first line antifungal agents were adjusted to second line agents due to their adverse effects in more than half of IPA episodes in the present study, more safe and effective antifungal therapy is expected in the future in Korea. Voriconazole treatment was associated with improved survival and fewer side effects compared to amphotericin B deoxycholate treatment of IPA (9), and empirical antifungal therapy with voriconazole was reported to be more economical than empirical therapy with amphotericin B deoxycholate (3839). In the present study, almost all IFD cases were IPA and no cases of mucormycosis were reported. In addition, in the IPA group of the present study, children who died received voriconazole therapy later than children who survived, although this difference was not statistically significant. Considering these results, voriconazole as well as liposomal amphotericin B and caspofungin could be considered as a first line antifungal agent in immunocompromised Korean children at risk for IPA to further improve prognosis in those children.
This study has several limitations including its retrospective nature. Cases of IFDs other than IPA were not thoroughly reviewed in the whole population of children with hematologic/oncologic diseases in our hospital. Risk factors for mortality and poor prognosis in children with IPA could not be evaluated due to the small number of children diagnosed with IPA. The enrolled children were heterogeneous - children with various types of underlying diseases were included and children receiving autologous or allogeneic HCT and not receiving HCT were included together. To overcome these limitations, a multicenter study including many children should be performed in the future.
In conclusion, 14.0% of children who received empirical antifungal therapy were diagnosed with IPA. Although amphotericin B deoxycholate was administered as a first line antifungal agent in most cases, mortality at 12 weeks after antifungal therapy was lower than previously reported in Korea. This improvement in prognosis of IPA was assumed to be arisen from early diagnosis of IPA. Therefore, early use of chest CT to identify halo signs in immunocompromised children who are expected to have prolonged neutropenia can be helpful for early diagnosis of IPA and improving prognosis of children with IPA. In addition, the prognosis of IPA in immunocompromised children is expected to be improved with the introduction of liposomal amphotericin B and caspofungin as first line antifungal agents in the future in Korea.



 XML Download
XML Download