

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hepatic injury after external beam radiotherapy (EBRT) to the liver was first described in the early 1960s; its clinical symptoms comprised rapid weight gain, an increase in abdominal girth, hepatomegaly, occasionally ascites or jaundice, and an elevation of liver enzymes, particularly serum alkaline phosphatase (1). The underlying pathology was identified as veno-occlusive disease, and this has become a classic model of radiation-induced liver disease (RILD) (2). Notwithstanding these clinical and pathological studies on RILD, EBRT has played a limited role in the treatment of liver cancers due to technical barriers over the past 30 yr. With the introduction of 3-dimensional conformal radiotherapy (3D-CRT) in the 1990s, however, multiple beams that are not in the axial plane can spare adequate volumes of the normal liver, and the use of dose-volume histograms (DVHs) can quantify the dose delivered to the normal liver (3). These technological advances have expanded EBRT indications for liver cancers. RILD was subdivided into classic RILD and non-classic RILD, and hepatic toxicity after 3D-CRT has been fairly well established with these endpoints (4).
On the other hand, RILD rarely occurs after stereotactic ablative radiotherapy (SABR), which is a newly emerging treatment method to deliver a high dose to the target, utilizing either a single dose or a small number of fractions with a high degree of precision within the body (567). Therefore, the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) or the progression of Child-Pugh (CP) class have been used in evaluating hepatic toxicity after SABR. To date, a few studies have reported several predictors that affect hepatic toxicity after SABR using various fractionation schemes (891011121314). Considering that the main obstacle for safe application of SABR remains the unavailability of data that allow the unambiguous determination of the parameters for fractionation schemes and dose prescriptions, however, additional studies should be needed to establish hepatic toxicity (15).
Therefore, this study included SABR in only 3 fractionations to avoid the ambiguity that arises while converting total doses from different fractions to the biologically equivalent dose. We evaluated the incidence of hepatic toxicity in primary and metastatic liver cancers after SABR using 3 fractions, and identified the predictors for hepatic toxicity.
MATERIALS AND METHODS
Patient selection
For patients with unresectable hepatocellular carcinoma (HCC), we conducted a SABR dose-escalation study with 33-57 Gy delivered in 3-4 fractionations between 2003 and 2008, and a phase II SABR study with 60 Gy delivered in 3 fractionations between 2008 and 2011 (1617). We registered 108 consecutive patients and treated them using SABR with curative-intent (18). Among these, 86 patients received SABR using 3 fractions. During the same period, 73 patients with other primary liver cancers or liver metastases received curative-intent SABR in 3 fractionations using a similar tumor dose, and normal tissue constraints based on previous prospective studies: cholangiocarcinoma (23 patients), gall bladder cancer (3 patients), other primary liver cancers (2 patients), and liver metastases (45 patients) (1920).
To evaluate hepatic toxicity after SABR, we retrospectively reviewed the medical records of these 159 patients. Patients who met the following criteria were excluded from this study: 1) intrahepatic disease progression and/or application of additional treatment within 3 months after the completion of SABR (51 patients), 2) 2 sessions of SABR within 3 months (3 patients), 3) absence of blood test results within 3 months (20 patients), 4) loss of follow up (6 patients), and 5) absence of planning data (1 patient). The remaining 78 patients, treated with SABR using 3 fractions between 2003 and 2011, were included in this study.
SABR technique
SABR was administered using CyberKnife (n=50) or RapidArc (n=28). The simulation data were entered into CyberKnife planning system (Accuray Inc., Sunnyvale, CA, USA) or Eclipse treatment planning system (Varian Medical Systems, Palo Alto, CA, USA). Gross tumor volume (GTV) was identified and contoured by using axial computed tomography (CT) images. GTV was considered equal to clinical target volume. Planning target volume (PTV) was defined as GTV plus 4 mm in the longitudinal direction and GTV plus 2 mm in all other directions. Radiation doses were prescribed at 74%-84% isodose line of the maximum dose for the CyberKnife and at 90%-100% for the RapidArc in order to cover at least 95% of the PTV. We adopted the liver dose constraints that at least 700 mL of the normal liver volume (total liver volume minus PTV) had to received a total dose of <15 Gy (phase I) or <17 Gy (phase II) in HCC studies. The details of treatment have been described in our previous studies (1617).
Evaluation of hepatic toxicity
Before SABR, patients underwent physical examination, blood tests, and CT to assess baseline hepatic function and to evaluate the tumor extent. Every 1 to 3 months after the completion of SABR, patients underwent physical examination, blood tests, and CT to assess hepatic toxicity and to evaluate the tumor response. Hepatic toxicity was scored according to CTCAE v4.0 by analyzing the serum of aspartate transaminase, alanine transaminase, alkaline phosphatase, albumin, total bilirubin, and prothrombin time, and checking the presence of hepatic failure. We defined newly-developed hepatic toxicity ≥grade 2 in the absence of documented progressive disease within 3 months after the end of SABR as significant adverse events.
Analysis of parameters and statistics
To determine the clinical predictors for hepatic toxicity ≥grade 2, various clinical parameters such as age (<60 vs. ≥60 yr), sex (male vs. female), Eastern Cooperative Oncology Group (ECOG) performance status (1 vs. 2), origin (HCC vs. others), liver cirrhosis (yes vs. no), viral hepatitis (yes vs. no), baseline CP score (liver function before SABR, 5 vs. 6-8), SABR duration (3 vs. 4-10 days), PTV (≤47 vs.>47 mL), and normal liver volume (<1,000 vs. ≥1,000 mL) were analyzed as binary variables. To determine the dosimetric predictors for hepatic toxicity ≥grade 2, we analyzed rV5Gy (normal liver volume receiving <5Gy, reverse V5Gy), rV10Gy, rV15Gy, rV17Gy, rV20Gy, rV25Gy, rV30Gy, and rV35Gy as continuous variables. These dosimetric parameters were calculated from DVHs.
Patients were grouped according to the severity of hepatic toxicity (grade 0-1 vs. grade 2-3). Univariate logistic regression analysis was used to compare the clinical and dosimetric parameters between the two groups. In addition, we used the Hosmer-Lemeshow test to predict for the goodness of fit for statistically significant dosimetric parameters from the logistic regression analysis. A low value of the test statistic, and a corresponding high P value, indicated that there was good agreement between the observed and expected number of events. All significant clinical parameters and the most-predictive dosimetric parameter were evaluated by multivariate logistic regression analysis. All calculations were performed using the Statistical Package for the Social Sciences software version 13.0 (SPSS Inc., Chicago, IL, USA).
Ethics Statement
This study was approved by the Korea Institute of Radiological and Medical Sciences institutional review board (IRB No. K-1210-002-016). Our institutional review board waived the need for written informed consent for the participants because this study was retrospective in nature and did not infringe on the patients' rights to data anonymity prior to analysis.
RESULTS
Patient characteristics
The 78 patients were comprised of 53 males (68%) and 25 females (32%), ranging in age from 33 to 79 yr (median, 60 yr). The ECOG performance status was 1 in 73 patients (94%) and 2 in 5 patients (6%). Sixty-nine patients were diagnosed with primary liver cancers: 61 patients with HCC (79%), 6 with cholangiocarcinoma (8%), 1 with gallbladder cancer (1%), and 1 with neuroendocrine carcinoma of the liver (1%). Nine patients were diagnosed with liver metastases: 5 patients with colorectal cancer (7%), 1 with adenocarcinoma of unknown primary origin (1%), 1 with breast cancer (1%), 1 with squamous cell lung cancer (1%), and 1 with ovarian cancer (1%). Fifty-three patients (68%) had liver cirrhosis. Hepatitis-B virus (HBV) was present in 46 patients (59%) and hepatitis-C virus in 4 patients (5%). A baseline CP score of 5 was observed in 62 patients (79%), 6 in 10 patients (13%), 7 in 4 patients (5%), and 8 in 2 patients (3%). SABR doses ranged from 36 Gy to 60 Gy (median, 54 Gy). Thirty-five patients (57%) received SABR for 3 consecutive days, and 26 patients (43%) received the treatment over 4-10 days, owing to the interruption of a holiday or a weekend, or owing to technical problems with the radiation treatment machine. The median PTV was 32 mL (range, 3-271 mL). The median normal liver volume was 1,132 mL (range, 634-1,971 mL).
Hepatic toxicity ≥ grade 2
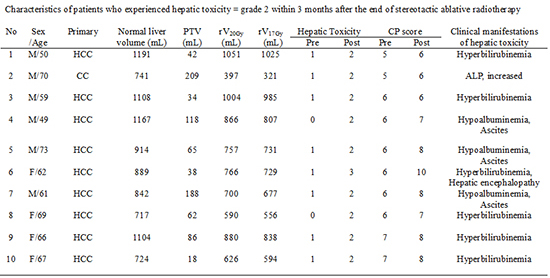
The characteristics of patients, who experienced hepatic toxicity ≥grade 2 within 3 months after the end of SABR, are shown in Table 1. Ten patients (13%) experienced hepatic toxicity ≥grade 2. The clinical manifestations of hepatic toxicity were hyperbilirubinemia, elevation of hepatic enzyme, hypoalbuminemia, ascites, and hepatic encephalopathy. Among these, 5 patients (6%) experienced the progression of CP class: from A to B in 4 patients; from A to C in 1 patient. Three patients with hypoalbuminemia of grade 2 were always accompanied with ascites of grade 2, which induced the progression of CP class. On the contrary, among the 5 patients with hyperbilirubinemia of grade 2, only 1 patient experienced the progression of CP class.
Predictors for hepatic toxicity
The results of the univariate analysis for clinical and dosimetric predictors affecting hepatic toxicity ≥grade 2 are summarized in Table 2 and Table 3. The baseline CP score, PTV, and normal liver volume were statistically significant clinical predictors. And all dose-volumetric parameters of rV5Gy-rV35Gy were statistically significant. The result of the Hosmer-Lemeshow test was not statistically significant (P=0.768), suggesting a good calibration of the models using these dose-volumetric parameters: among these, rV20Gy was the most significant predictor (P=0.013). On multivariate logistic regression analysis containing all significant clinical predictors according to univariate analysis and the most-predictive dosimetric parameter (rV20Gy), the baseline CP score (5 vs. 6-8) was the only significant predictor for hepatic toxicity ≥grade 2 (hazard ratio, 0.026; 95% confidence interval, 0.003-0.221, P=0.001). Fig. 1 shows DVHs of the normal liver from all patients. Patients with a CP score of 5 were tolerable although a larger volume of the normal liver was irradiated.
DISCUSSION
Hepatic toxicity is one of the most important toxicities when EBRT is applied to the liver. Historically, hepatic toxicity after conventional RT has been well documented as RILD. RILD typically occurred between 2 weeks to 3 months after conventional RT and the overall incidence of RILD was 7%-20% (421). However, RILD rarely occurred with≤5% of cases after SABR (46). In our study, RILD was found to occur in 1% of patients. In contrast to conventional RT, the low rate of RILD after SABR can be ascribed to three main reasons. First, there is a substantial difference in normal liver dose distribution. SABR has a lower mean dose and minimizes the delivered dose to larger volumes of the normal liver by maintaining steep dose gradients, while conventional RT includes large volumes of the normal liver even in high-dose regions (622). Second, high dose per fraction during SABR can induce endothelial damage, and consequently, reduced perfusion (23). This can result in diminished reoxygenation effects, unlike conventional RT, and affect different repair mechanisms on normal tissue (24). Finally, protracted dose delivery from SABR using gating method or intensity-modulated radiotherapy might allow the DNA repair processes to initiate before the entire RT dose is applied, increase survival especially in cells with a high repair capacity such as normal tissue, and decrease normal tissue toxicity (25). Therefore, SABR studies generally reported hepatic toxicity with other endpoints such as CTCAE criteria or the progression of CP class.
Table 4 and Table 5 present the hepatic toxicity by these endpoints from prospective or retrospective studies using SABR for primary and metastatic liver cancers (89101112131426272829). The overall incidence of hepatic toxicity was varied from 0% to 33%; our study reported an incidence of 13% for hepatic toxicity ≥grade 2 and 6% for the progression of CP class. Prospective studies, in which patients had good baseline liver function and where a definite liver dose constraint (rV15Gy ≥700 mL: generally recommended liver dose constraint) was met in all patients, reported no hepatic toxicity as shown in Table 4. On the other hand, Table 5 shows that hepatic toxicity occurred when definite liver dose constraints could not be strictly satisfied, regardless of the type of constraint. In the current study, the constraint of rV17Gy ≥700 mL was met in 65 patients: 6 patients (9%) experienced hepatic toxicity ≥grade 2; and 3 patients (5%) experienced the progression of CP class. On the other hand, rV17Gy of 13 patients was below 700 mL: 4 patients (31%) experienced hepatic toxicity ≥grade 2; and 2 patients (15%) experienced the progression of CP class. Therefore we should set a definite liver dose constraint and should conduct SABR to the liver under a well-organized clinical setting, even though the optimal liver dose constraint remains unknown because of the small number of patients and heterogeneity in origin, tumor sizes, baseline liver functions, and the number of fractions. In cases where the liver dose constraint is not met, dose per fraction would be reduced or the number of fractions would be increased. This might mean the conversion from SABR into hypofractionation or conventional fractionations considering that sequential phase I and II trials of SABR for HCC patients with a baseline CP class of A, in which they used 6 fractions and prescribed relatively lower total doses (median 36 Gy), reported a 29% decline of CP class at 3 months after SABR (30).
Table 5 also shows the several predictors for hepatic toxicity after SABR. Several clinical and dosimetric predictors were involved in the development of hepatic toxicity. Among these studies, 5 studies including our study indicated that the baseline CP score was the most important predictor: 3 studies suggested that baseline CP scores ≥8 is not safe for SABR (81014). A recent study which conducted SABR for HCC patients with CP class of B or C reported the highest incidence of hepatic toxicity 63% at 3 months after end of SABR (31). They found that treatment of patients with a CP class of B was not without risk of toxicity and suggested SABR as a treatment option for selected HCC patients with modestly impaired liver function (a baseline CP score of 7). On the other hand, our study showed that 2 patients with a baseline CP score of 8 did not experience hepatic toxicity ≥grade 2. Although these patients had normal liver volumes of 754 mL and 634 mL due to underlying liver cirrhosis related to HBV, they had small PTVs (11 mL and 10 mL) and SABR plan was conducted to minimize the irradiation dose to the normal liver: rV17Gy was 724 mL and 588 mL. Fig. 1 shows that these 2 patients received the lowest irradiation doses to the normal liver. Thus, SABR may be conditionally employed in patients with a baseline CP score of 8, only if the irradiation dose to the normal liver can be minimized. Otherwise, an increase of the number of fractions should be considered. In patients with a baseline CP score of 5, SABR to the liver would be considered as a safe treatment method. Among the 62 patients with a baseline CP score of 5 in this study, only 2 patients (3%) experienced hepatic toxicity of grade 2, without the progression of CP class. Fig. 1 represents patients with a baseline CP score of 5 who were tolerable in irradiation of higher doses to the normal liver than patients with baseline CP scores of 6-7. Therefore, SABR to the liver is a safe treatment option for patients with a baseline CP score of 5 based on the current liver dose constraint; however, further studies are needed to establish optimal liver dose constraint to minimize hepatic toxicity for patients with baseline CP scores of 6-7.
There were some limitations in the current study. First, this study was a retrospective analysis. Therefore, selection bias may have occurred, and the rate of hepatic toxicity may have been underestimated. Second, low incidence of hepatic toxicity was included although this study is one of having the largest number of patients and a fixed regimen of 3 fractions among the published studies focused on SABR. Therefore, we conducted statistical analysis with an endpoint of hepatic toxicity ≥ grade 2. However, hepatic toxicity ≥grade 2 would not generally lead to severe radiation-induced morbidity or mortality in the long term (9). In our study, most patients with hepatic toxicity ≥ grade 2 did not experience further deterioration in hepatic function. Considering that many studies for SABR to the liver did not report an evaluable number of patients at follow-up and accurate ratios of patients with hepatic toxicity, our study using CTCAE criteria with consistency of reporting is meaningful.
In conclusion, SABR using 3 fractions to primary and metastatic liver cancers produces acceptably low hepatic toxicity. On multivariate analysis, the baseline CP score (5 vs. 6-8) is the only significant predictor. Further studies should establish optimal liver dose constraint to minimize hepatic toxicity, especially in patients with baseline CP scores ≥6.



 XML Download
XML Download