

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
An awareness of the clinical demographics and outcomes of mechanically ventilated patients in the intensive care unit (ICU) is important because it allows for better use of resources and helps in clinical decision making (1, 2, 3). Moreover, it is important to know local epidemiologic data, because available resources vary from country to country (4, 5, 6), but few data are available in Korean patients.
A group led by Esteban A., has been conducting surveys on mechanical ventilation periodically since 1998 (1, 2). The third international survey was conducted in 2010 (3) and, for the first time, 12 Korean ICUs participated in this large prospective cohort study. The present study provides analysis of data from 12 Korean ICUs and describes the current status of mechanically ventilated patients in Korea.
MATERIALS AND METHODS
Patients
Consecutive adult patients (age ≥ 18 yr), who received mechanical ventilation for longer than 12 consecutive hours or non-invasive ventilation (NIV) for more than 1 hr during a 1-month period starting on 1 March, 2010, and ending on 31 March, 2010 (3), from participating ICUs of 12 university hospitals in Korea, were included in this study. A full list of participating centers can be seen at the Acknowledgement section of this paper.
Data collection
Only the investigator and research coordinator in each ICU were aware that the study was underway, to minimize any changes of behavior as a result of being observed. Each center was provided with a manual describing data collection methods and definitions used in the study.
The following information was collected from each patient: age, sex, weight, height, Simplified Acute Physiology Score II (SAPS II) at ICU admission, reason for initiation of mechanical ventilation, and arterial blood gas analysis at the start of mechanical ventilation. The following data and events were assessed daily during the course of mechanical ventilation for a maximum of 28 days: modes of mechanical ventilation; ventilator settings; co-adjuvant therapy (sedatives, analgesics, neuromuscular blockers, intensive insulin therapy, steroids, and prone position); complications (sepsis, need for renal replacement therapy, acute respiratory distress syndrome [ARDS], ICU-acquired pneumonia, barotraumas, and development of each organ failure, defined as ≥ 3 points of sequential organ failure assessment [SOFA] score for that organ); and clinical outcomes (duration of mechanical ventilation and weaning, re-intubation, tracheostomy, length of stay in ICU and hospital, and ICU and hospital mortality).
The use of sedatives, analgesics, and neuromuscular blockers was recorded when these medications were given for ≥3 hr during a 24-hr period. Conventional definitions for sepsis (7), ARDS (8), pneumonia (9), and organ failure (10) were used as described previously. Barotrauma was defined as pneumothorax, pneumomediastinum, pneumoperitoneum, and subcutaneous emphysema, which was thought to be related to mechanical ventilation. The duration of mechanical ventilation was calculated as the time between the initiation of mechanical ventilation and the date of extubation or ICU discharge (when the patient was referred to another hospital or had died). All patients were followed up until hospital discharge.
Statistical analysis
All data are presented as the medians (interquartile range [IQR]) or means (standard deviation [SD]) for the continuous variables and as numbers (percentages) for the categorical variables. The present data do not fit a normal distribution. However, we presented some data as mean and SD to enable comparison with previous data that are presented using these measures of central tendency. Some continuous variables, such as tidal volume per predicted body weight (TV/PBW) and positive end-expiratory pressure (PEEP), were coded as dummy variables, using cut-off points based on published threshold values. The data on initial ventilator settings were compared using Kruskal-Wallis test. When there was statistically significant difference, Mann-Whitney test with Bonferroni adjustment was used to identify between which groups had the difference.
A multiple logistic regression analysis with backward stepwise selection method was used to identify independent prognostic factors that were associated with ICU mortality. The criterion for entering variables was if P value is < 0.20 in the univariate logistic regression. All of the statistical analyses were performed using PASW Statistics 18.0 (SPSS Inc., Chicago, IL, USA); a two-sided P<0.05 was considered significant.
Ethics statement
The study protocol was reviewed and approved by the institutional review board (IRB) of each hospital (Asan Medical Center, IRB No. 2010-0224; Samsung Medical Center, IRB No. 2010-03-079; Chungbuk National University School of Medicine, IRB No. 2010-04-019; Yonsei University College of Medicine, IRB No. 4-2010-0110; Ewha Woman's University School of Medicine, IRB No. 224-2; Korea University Ansan Hospital, IRB No. AS10028; Pusan National University Yangsan Hospital, IRB No. 02-2010-024; Dongguk University Gyeongju Hospital, IRB No. 10-05; Catholic University of Daegu Hospital, IRB No. CR-10-020; Hallym University Sacred Heart Hospital, IRB No. 2010-16; and Yonsei University Wonju Severance Christian Hospital, IRB No. 2009-03), and the need for consent was waived because of the non-interventional nature of the protocol.
RESULTS
Baseline characteristics
The baseline characteristics are shown in Table 1. Overall, 275 patients were enrolled. The median (IQR) age was 69 (54-75) yr. The common reasons for initiation of mechanical ventilation were pneumonia (23%), acute respiratory failure on chronic pulmonary disease (ARF-CPD, 16%), sepsis (10%), and ARDS (10%). Most of the patients received mechanical ventilation because of medical problems, except for 5% of the population who had surgical problems (patients with postoperative acute respiratory failure [n=12] and trauma [n=2]).
Mode and setting of mechanical ventilation
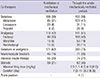
Fig. 1 shows the initial ventilator settings according to each major reason for initiating mechanical ventilation. Median TV/PBW for all patients was 7.4 (6.2-8.8) mL/kg. The value for patients with ARDS was 6.4 (5.7-7.7) mL/kg; however, there was no statistically significant difference between the two groups. Median PEEP for all patients was 6 (5-8) cmH2O. Patients with ARDS (10 [6-12] cmH2O) received higher PEEP than those with pneumonia (6 [5-8] cmH2O, P=0.006) and ARF-CPD (5 [4-8] cmH2O, P<0.001). Median peak pressure for all patients was 24 (19-28) cmH2O. Patients with ARF-CPD (27 [22-32] cmH2O) had higher peak pressure than those with pneumonia (23 [19-26] cmH2O, P=0.030).
Fig. 2 shows the number of patients ventilated (gray bar) and percentage of each ventilator mode (line graph) in all patients over time. Pressure control ventilation (PCV) mode was the preferred mode initially (40%) and was most preferred during the entire period of mechanical ventilation. Volume assist/control (A/C) mode was the second most common mode initially but the percentage of patients ventilated with this mode decreased with time. More and more patients were ventilated using pressure support ventilation (PSV) mode as the number of days on the ventilator increased.
Co-adjuvant therapy
The co-adjuvant therapies are listed in Table 2. Sedatives of any type were administered in 155 patients (56%), analgesics in 141 (51%) patients, and neuromuscular blockers in 71 (26%) patients. Midazolam and fentanyl were the preferred sedative and analgesic drugs, respectively.
Clinical courses and outcomes
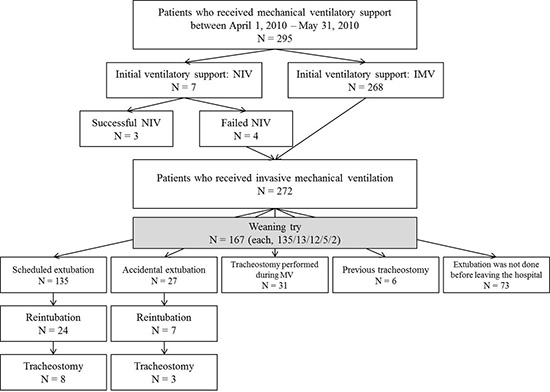
Clinical course of mechanical ventilation is shown in Fig. 3. NIV as initial ventilator support was attempted in only seven patients (2%). Only three patients were successfully managed with solely NIV. Of 272 intubated patients, 135 (50%) patients were able to be extubated electively. Of these 135 patients, 24 (18%) patients were re-intubated. Of 272 intubated patients, the incidence rate of accidental extubation was 10% (27 cases/272 patients), and incidence density of that was 1.1% (27 cases/2,457 ventilator days). Of these 27 patients, seven (26%) patients were re-intubated. Of 162 patients who underwent extubation before tracheostomy, 31 (19%) patients underwent re-intubation at a median of 11 (1-38) hr after extubation. The reasons for re-intubation in these patients were: increased work of breathing (n=15), large amounts of secretions (n=6), neurologic problems (n=5), upper airways obstruction (n=3), and congestive heart failure (n=1). Excluding those patients admitted to the ICU with a tracheostomy tube in situ, 42/266 (16%) patients underwent tracheostomy during their course of ventilation within a median of 13 (9-18) days after intubation.
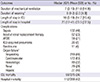
Clinical outcomes and complications are listed in Table 3. The median total duration of mechanical ventilation was 7 (3-13) days and the median length of stay in ICU was 10 (5-19) days. Various complications and organ failures occurred. The median number of failed organs was 2 (1-3). ICU mortality was 36%.
Prognostic factors for ICU mortality
Table 4 lists both univariate and multivariate analysis of factors associated with ICU mortality in mechanically ventilated patients. The multiple logistic regression model revealed that the SAPS II score at ICU admission (odds ratio [OR], 1.034; 95% confidence interval [CI], 1.001-1.036; P=0.033), peak pressure (OR, 1.054; 95% CI, 1.016-1.095; P=0.006), and the number of failed organ (OR, 2.132; 95% CI, 1.634-2.781; P<0.001) were independently associated with ICU mortality.
DISCUSSION
This paper analyzes data that forms the Korean contribution to an international study (3). There were several differences in clinical outcome between the results of the international study and Korean data for the cohort of 2010 (see Table S1 in the online supplement). In the Korean data, the mechanically ventilated patients underwent fewer scheduled extubations (50% vs 57%), more re-intubations (18% vs 12% in patients with a scheduled extubation; and 26% vs 20% in those with an unplanned extubation), a higher incidence of complications (63% vs 39%, incidence of cardiovascular failure; 32% vs 8%, incidence of hematologic failure; 48% vs 18%, incidence of sepsis; and 21% vs 6%, incidence of ARDS), a longer duration of mechanical ventilation (7 [3-13] days vs 5 [3-10] days) and length of stay in ICU and hospital, and finally had higher ICU mortality (36% vs 28%) and hospital mortality (42% vs 35%) compared with the international cohort (3). These differences in the outcomes appear to derive from differences in the composition of the participants studied. In our Korean data, the patients had a higher SAPS II score at ICU admission (52±18 vs 45±18) and mechanical ventilation was required for medical reasons (23% vs 10%, pneumonia; 10% vs 3%, ARDS; and 4% vs 21%, postoperative) more frequently compared with the international cohort (3). As for co-adjuvant therapy, sedatives (56% vs 71%) and analgesics (51% vs 62%) were less commonly used and neuromuscular blockers (26% vs 11%) were more commonly used in Korea. Regarding the initial ventilator settings, the most important finding was that the use of NIV was parsimonious in Korea: NIV was used as the first ventilator mode of ICU admission in only 2% of total ventilated patients in Korea, which is much lower than that of international survey (14%) (3). The usefulness of NIV is well known in patients with acute exacerbation of chronic obstructive pulmonary disease (11), or with cardiogenic pulmonary edema (12), and in immunocompromised patients with acute respiratory failure (13). However, the low use of NIV may be attributed to the low nurse-to-patient ratio in Korea and inadequate reimbursement from the government compared with invasive ventilation (6). With regards to the ventilator modes used each day, increased use of PSV mode and decreased use of volume A/C mode, as the number of days on a ventilator increased, were observed in both the Korean and the international cohorts (see Fig. E1 of reference 3). PCV mode was the most popular mode of ventilation in Korea, applied to 35%-50% of patients. In the international data, however, the PCV mode was a less popular mode of ventilation, applied to 10%-20% of patients.
Compared with previous Korean data (5, 6, 14), there are several differences in ventilator management; for example, increased favor of the pressure mode, a decrease in tidal volume, and an increase in applied PEEP. These trends are similar to those reported in international surveys (1, 2, 3). Initial ventilator modes were PCV in 40% of patients and volume A/C mode in 31% of patients in the 2010 Korean cohort. In particular, PCV and volume A/C mode were used in 56% and 22% of patients with ARDS, respectively. These findings differ from those of the 2003 Korean cohort, which reported preferred use of the volume A/C mode in 43% of all patients and 45% of ARDS patients, respectively (6). In the present cohort, the initial ventilator settings were TV/PBW of 7.7±2.3 mL/kg and PEEP of 6.5±3.3 cmH2O, which were slightly lower (TV/PBW) and higher (PEEP) compared with the 2003 cohort (8.1±2.1 mL/kg and 5.0±3.8 cmH2O, respectively) (5). Patients with ARDS in the 2010 cohort received initial ventilator settings of TV/PBW=7.0±2.0 mL/kg and PEEP = 9.2±3.8 cmH2O. Compared with the 2003 cohort, the TV/PBW is lower, while the PEEP is no different (7.6 mL/kg and 9.4 cmH2O without presented SD, respectively) (6). This trend to lower the TV/PBW for ARDS patients may have been influenced by several randomized trial results, which concluded that a lower TV/PBW was associated with lower mortality (15, 16). However, the use of NIV was still low in both the 2003 and 2010 cohorts (4% and 2%, respectively) in Korea (5, 6).
Another noticeable change over time has been in the use of sedatives, analgesics, and neuromuscular blockers. In the present cohort, 21%, 35%, and 26% of the patients were administered sedatives only, a combination of sedatives and analgesics, and neuromuscular blockers, respectively. In the 2003 cohort of Korea, 50%, 22%, and 41% of the patients received sedatives only, a combination of sedatives and analgesics, and neuromuscular blockers, respectively (14). That means that the strategy of analgesia-based sedation, which was recently recommended over the strategy of hypnotic-based sedation (17, 18), was used more frequently, while neuromuscular blockers, which can cause critical illness polyneuropathy/myopathy (19), were used less frequently. Although there were no data recording the incidence of delirium or the use of antipsychotics, these results could be interpreted as an improvement in strategy and the appropriate use of sedatives and analgesics for the management of mechanically ventilated patients.
There are no multicenter data available in Korea to compare the incidence of complications occurring while patients are mechanically ventilated compared with the international cohort (1, 3). Of these complications, according to multivariate analysis in our study, organ failure was associated with ICU mortality. This finding suggests that preserving the function of damaged organs is important in the management of mechanically ventilated patients. ICU mortality was 36%, unchanged from the findings of the 2003 cohort of Korea (28-day mortality, 41%) (6).
This study has several limitations. First, comparisons between the present data and previous reports may be influenced by bias originating in differences of methodology. Hong et al. performed a 1-day point-prevalence study (5), while Koh et al. conducted a survey of patients who received mechanical ventilation for more than 72 hr (6). Second, there may be large discrepancies between data from each participating hospital because of differences in their available resources. Therefore, caution is required before applying these results to the practice of other hospitals.
This report is a snapshot showing the current use of mechanical ventilation in Korea. NIV is still used infrequently. Some changes were seen in the management of mechanically ventilated patients, which could be interpreted as the acceptance of recently recommended practice. However, high mortality was still observed in this cohort. Based on this report, we need further clinical trials of ventilator strategies to improve the mortality of mechanically ventilated patients.





 XML Download
XML Download