

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Chronic sputum is a troublesome symptom that occurs in many respiratory diseases. It is associated with an accelerated decline in lung function, increased hospitalization (1), and an increase in all-cause mortality (2). The prevalence of chronic cough and sputum production consistently augment with increasing airflow limitation (3). A few reports underline that chronic cough and sputum production before airflow obstruction can offer a unique opportunity to identify subjects at risk for chronic obstructive pulmonary disease (COPD) for an early intervention (4). Chronic sputum has been recognized as a result of tobacco smoking and exposure to industrial dusts or fumes. Other causes of chronic sputum include many respiratory diseases, such as COPD, lung cancer, respiratory tract infection, bronchiectasis, etc. (5, 6, 7). Prevalence of chronic sputum varies from 1.2 to 13% according to the country (2, 8, 9, 10). However, there are a few studies that assess the prevalence and risk factors of chronic sputum production in the general population, but no report about the prevalence and risk factors of chronic sputum in Korea.
This study was planned to estimate the prevalence of chronic sputum and to study its associated factors in a general Korean population aged over 40 yr.
MATERIALS AND METHODS
Study design and measurement
This study collected information from the first and second periods of the 5th Korea National Health and Nutrition Examination Survey (KNHANES V) 2010 and 2011. KNHANES is a cross-sectional survey that consists of a health interview, a health behavior questionnaire, a health examination, and a nutrition survey for the general population of Korea (11, 12, 13, 14). KNHANES subjects include a representative national sample of the Korean population who were selected using a complex, stratified, multistage probability cluster sampling design (12, 13, 14). Participants in KNHANES are non-institutionalized civilians. A total of 17,476 people participated in KNHANES V in 2010 and 2011.
Because the spirometry and respiratory questionnaire were not performed on adults aged <40 yr who participated in the KNHANES (15), the sample for this study was limited to adults aged ≥40 yr. The subjects eligible for the present study were those who 1) participated in the KNHANES V and aged ≥40 yr old, 2) had lung function measurements, 3) had a response to the question: "Have you had sputum almost every day at least three consecutive months one year?". Demographic data selected from KNHANES V included age, gender, level of education, occupation, type of house, smoking status, pulmonary function test, and tuberculosis.
Chronic sputum was defined as daily emission of sputum that lasted for at least 3 months a year, for more than 1 yr (16). Tuberculosis included both current tuberculosis and past history of tuberculosis. Airflow obstruction was defined as a ratio of the forced expiratory volume in 1 second (FEV1) to the forced vital capacity (FVC) less than 0.7, using data from pre-bronchodilator test. COPD was defined as airflow obstruction in persons aged ≥40 yr (17). The smoking status was classified as never smokers, past smokers or current smokers (<15 pack-years "light smokers," ≥15 pack-years "moderate-heavy smokers"). Never smokers were defined as subjects who had never smoked. Past smokers were defined as subjects who stopped smoking at least in the last year, and current smokers were defined as subjects who continued to smoke (10). Age was categorized into four classes. Occupation was classified into seven categories: managers and professionals, clerks, service and sales workers, skilled agricultural, forestry and fishery workers, plant and machine operators and assemblers, elementary occupations, and unemployed.
Statistical analysis
The data analysis was carried out utilizing SPSS version 18 to estimate the prevalence of chronic sputum and to evaluate the associated factors for chronic sputum. The dummy variable approach was used to derive the odds ratio for each of the variables, which were of categorical nature, such as age, occupation, and education. The dummy variables were prepared considering each of the classification within the variable as a separate "risk factor" and the remaining subjects as "no risk factor." The multivariate analysis was carried out to study the independent association of the factors, which were observed to be significant in the univariate analysis. Differences in pulmonary function parameters between subjects with and without chronic sputum were examined using independent t-test.
Ethics statement
This investigation was conducted according to the principles expressed in the Declaration of Helsinki. All examination protocols were approved by the institutional review board of the Korea Centers for Disease Control and Prevention (No. 2010-02CON-21-C and No. 2011-02CON-06-C) (11). Informed consent was waived by the board.
RESULTS
In the 2010-2011 KNHANES V, 9,159 subjects aged ≥40 yr were included. Among them, 2,317 subjects did not undergo spirometry and 59 were excluded because of missing or inadequate answer to the question for chronic sputum. A total of 6,783 subjects were eligible for the present study: 430 with chronic sputum, 6,353 without chronic sputum (Fig. 1).
Characteristics of the sample population are presented in Table 1. Of 6,783 participants, 3,002 (44.3%) were men. The mean age of the participants was 57 yr (range: 40-97). More than half of the subjects lived in non-apartment. Most of the males were smokers (2,539, 85.3%), whereas most of the females were never smokers (3,473, 92.5%). Among smokers, moderate to heavy smokers were more than light smokers. The prevalence of COPD was 12.9%, higher in men (21.5%) than in women (6.0%). The number of subjects with current tuberculosis treatment or a history of tuberculosis was 391 (5.8%).
The prevalence of chronic sputum in the population studied was 6.3% (n=430). Among the subjects with chronic sputum, 24.0% (n=103) had a chronic cough. The prevalence of sputum and its associated factors are presented in Table 2. The prevalence of chronic sputum was higher in men than in women (OR, 2.517; 95% CI, 2.051-3.089), was positively associated with age (≥70 yr) (OR, 1.808; 95% CI, 1.355-2.411), and was higher in both past and current smokers than in never smokers (OR, 1.675; 95% CI, 1.284-2.186, OR, 4.378; 95% CI, 3.489-5.493, respectively), especially in moderate to heavy smokers (OR, 3.488; 95% CI, 2.803-4.340). Also, COPD and tuberculosis were associated with an increased risk of chronic sputum (OR, 2.580; 95% CI, 1.991-3.342, OR, 2.266; 95% CI, 1.650-3.111, respectively). The level of education, occupation, and type of house were not associated with a risk of chronic sputum.
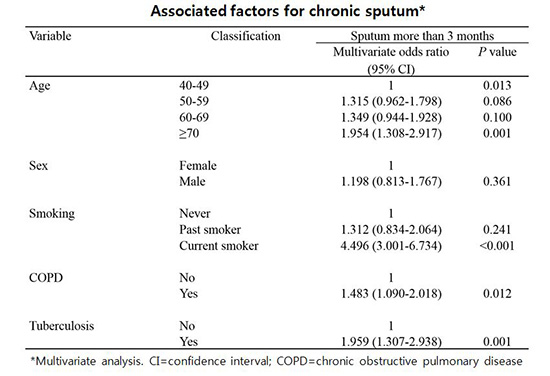
The multivariate logistic regression analysis was carried out to find the independent factors associated with chronic sputum (Table 3), utilizing the factors that were significant in the univariate analysis. Independent association with chronic sputum was observed for age, COPD, tuberculosis, and smoking, but not for gender. Because odds ratio for chronic sputum increased with age, the older age groups had higher risk. Regarding smoking status, current smoking was a significantly associated factor for chronic sputum.
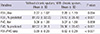
Pulmonary function parameters between subjects with and without chronic sputum are shown in Table 4. Compared with subjects without chronic sputum, significant reduction of FEV1 (% predicted), FVC (% predicted), and FEV1/FVC ratio were found in subjects with chronic sputum (P<0.001).
DISCUSSION
The present study evaluated the prevalence of chronic sputum and its associated factors in a general Korean population. The prevalence of chronic sputum was 6.3%. Older age, COPD, tuberculosis, and current smoking were independently associated with chronic sputum. Previous studies from other countries reported that the prevalence of chronic sputum varied from 1.2 to 13% (2, 8, 9, 10). In a cross-sectional survey by Mahesh et al. (10), the prevalence of chronic sputum was found to be 1.2% in India, and significant association was observed between chronic sputum, age, and smoking in 4,333 adults aged more than 40 yr living in the rural area of India. In another cross-sectional survey by Cerveri et al. (8), the prevalence of chronic sputum was 11.9% in Italian people aged between 20-44 yr, and the survey showed that gender (female), smoking, and low socioeconomic status were significantly and independently associated with chronic cough and sputum, with current smoking being the major associated factor. The prevalence of chronic sputum in the present study was in the intermediate range (6.3%) compared with other countries.
Increasing age was found to be an important factor associated with chronic sputum in our study, probably reflecting a higher prevalence of diseases associated with chronic sputum, like bronchiectasis, and a longer duration of exposure to other risk factors. The prevalence of chronic sputum of 8.7% seen in subjects above 70 yr was less than the prevalence observed in another study (2) that included subjects above 65 yr, but more than that in the Indian study (10).
Current smoking was found to be an important association identified in this study for chronic sputum, and both light and moderate to heavy smokers had a higher prevalence of chronic sputum than never smokers. A dose response relationship (association between amount of smoking and chronic sputum) was observed in multivariate analysis, when the amount of smoking was included as a variable (data not shown). Previous studies (8, 10, 18) have demonstrated that smoking is a major risk factor for many respiratory diseases and symptoms with a dose-response relationship. This supports that smoking is an important factor for chronic sputum irrespective of geographical location as well as other smoking-related diseases (10, 19, 20), and that smoking cessation should be encouraged in subjects with chronic sputum to relieve their symptoms.
COPD was significantly associated with chronic sputum. It is well known that chronic sputum is one of common symptoms in COPD (5). Chronic mucus hypersecretion was considered as a marker of airway inflammation (1, 21). Sputum production has been shown to associate with cellular and structural components of inflammation in COPD (22). Also, it has been considered as an important indicator of respiratory morbidity and mortality. Vestbo et al. (1) reported that chronic cough and sputum production were associated with an excessive FEV1 decline and increased risk of hospitalization because of COPD. These symptoms were associated not only with increased mortality risk (23, 24) but also with exacerbations of COPD (16, 25).
Current tuberculosis or history of tuberculosis was independently associated with chronic sputum in the present study. We speculated that these are probably due to inflammation of respiratory tracts, complication of tuberculosis, such as bronchiectasis (26), extensive pulmonary destruction (26, 27), and chronic pulmonary aspergillosis (28). Other risk factors or diseases can be also responsible for chronic sputum in the community. For instance, underlying respiratory diseases, such as rhinitis, sinusitis, asthma, bronchiectasis, or cystic fibrosis can cause chronic sputum by increasing mucus production (29, 30, 31). Moreover, comorbidities such as gastroesophageal reflux, diabetes, cerebrovascular disease, neuromuscular disease can cause chronic sputum by increasing risk of pulmonary aspiration (32, 33). In addition, biomass fuel exposure in rural area is associated with diverse respiratory disease that can cause chronic sputum (34). However, KNHANES V did not obtain enough information about various underlying respiratory diseases and comorbidities. This is one of our study limitations.
Accompanying symptoms of chronic sputum, such as chronic cough, increasing dyspnea, and increased sputum volume/purulence should be investigated, because these symptoms can provide important clinical information about pathology in the bronchopulmonary system (29, 35). However, we could not describe other symptoms except chronic cough, because KNHANES V did not obtain information about other respiratory symptoms. This is another limitation of this study.
Baseline dermographic characteristics of all subjects aged ≥40 yr in KNHANES V were similar to those finally included in the present study. In addition, age, tuberculosis, smoking, and COPD were also significant risk factors for chronic sputum when we analyzed the data from all participants in KNHANES V. These results suggest that sample selection bias was not meaningful in this study.
This study has several limitations. First, we could not evaluate all age group because the spirometry and respiratory questionnaire were performed only on adults aged ≥40 yr. Second, KNHANES V did not obtain enough information about underlying respiratory related diseases, comorbidities, and accompanying symptoms that can be related with chronic sputum as mentioned in the above paragraphs. There is a need for studies to identify more various diseases and factors other than COPD and tuberculosis responsible for chronic sputum in the community. Finally, given the cross-sectional nature of the surveys, we were unable to determine causal relationships between chronic sputum production and other independent variables. Their causal relationship should be verified in future longitudinal studies. Despite these limitations, this study has powerful strength, because the subjects of the current study are representative of the general Korean population.
In conclusion, our findings demonstrate that the prevalence of chronic sputum in the Korean general population is in the intermediate range compared to other countries. Current smoking is an important preventable risk factor identified in this study, and efforts towards smoking cessation are important for respiratory health. Furthermore, major respiratory diseases, such as COPD and tuberculosis, should be considered in subjects with chronic sputum.

 XML Download
XML Download