

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Intradialytic hypotension (IDH) occurs in 15%-60% of the treatments (1, 2, 3). It is usually associated with symptoms of nausea, dizziness, cramps, fatigue and weakness, which significantly diminishes patient's quality of life and tolerability to dialysis (2). It also limits fluid removal, which leads to volume overload and interferes with the delivery of an adequate dialysis dose (2). It causes myocardial ischemia and dysfunction and results in increased mortality in hemodialysis (HD) patients (2, 4, 5). Therefore, IDH remains a challenging problem in the management of HD patients.
The etiology of IDH is multifactorial. The primary factor of it seems to be the reduction of circulating blood volume due to massive ultrafiltration (UF) and sodium removal and subsequent imbalance between UF rate and plasma refilling rate. Impaired cardiovascular compensations for reduced circulating volume, which include increased cardiac output and contractility and increased peripheral vascular resistance also contribute to the development of IDH (1, 2, 6).
Common strategies that prevent IDH include accurate and frequent assessment of dry weight, patient education to avoid excessive interdialytic weight gain, no heavy meals during dialysis, adequate hypertension management, sodium and UF profiling, cool dialysate temperature, use of dialysate containing bicarbonate buffer or high concentration of calcium, pharmacologic measures including α1-adrenergic agonist, and convective therapies including hemofiltration and hemodiafiltration (2, 7, 8, 9, 10, 11, 12, 13, 14).
Automatic biofeedback system is a unique technology that may reduce IDH. The Hemocontrol function evaluates the blood volume reduction curve during HD and continuously adjusts the UF rate and the dialysate conductivity to make that blood volume curve follows a predefined trajectory, which offers the best condition for hemodynamic stability in response to fluid removal. This system has been evaluated in clinical trials with variable success in reducing IDH or cardiovascular morbidity (15, 16, 17, 18, 19).
We conducted a multicenter prospective crossover study to determine whether Hemocontrol biofeedback system (HBS) reduces the frequency of IDH in hypotension-prone HD patients compared with conventional HD.
MATERIALS AND METHODS
Study population
Potential participants were screened at 9 centers according to our definition of IDH, which was a decrease in systolic blood pressure (BP)≥20 mmHg or a decrease in mean arterial pressure (MAP)≥10 mmHg during HD associated with clinical events and need for nursing interventions. Inclusion criteria were chronic HD patients on 3 times a week schedule for >3 months, frequency of IDH>25% of treatment sessions during last 1 month preceding the study, age 18-74 yr, ability to provide consent, and interdialytic weight gain>1.5 kg. Exclusion criteria were pre-dialysis MAP in supine position<90 mmHg, delivered blood flow rate for dialysis<200 mL/min, pre-dialysis hemoglobin level>13 g/dL, treatment by hemodiafiltration, unstable angina, myocardial infarction, decompensated congestive heart failure, hemodynamically important valvular heart disease in past history and expected need for blood transfusions.
Study design
This multicenter prospective crossover study consisted of period A (8 weeks), period B0 (2 weeks), and period B1 (8 weeks). During period A, conventional HD was performed 3 times a week, 4 hr per treatment and using a bicarbonate dialysate. Each patient used same dialyzer during the entire study period. Patient's dry weight was decided by the clinical and radiological assessment. Period B0 is a preparation phase for period B1, which required for establishing the patient's individual blood volume (BV)/UF volume values that are required as input to Hemocontrol. The BV sensor (Hemoscan™, Gambro, Dasco S.p.A., Italy) connected to dialysis machine (Artis Dialysis System, Gambro, Dasco S.p.A., Italy) was activated, and constant UF rate and dialysate sodium were set throughout the HD treatment. Then, the BV curve shape and the BV/UF volume parameter required by Hemocontrol were assessed. During period B1, Hemocontrol was activated and BV/UF volume parameter was initially set as determined in period B0. The Hemocontrol function of the Artis dialysis machine evaluated the BV reduction curve during dialysis based on the variation of hematocrit levels, and continuously adjusted the UF rate and the dialysate conductivity to make that BV curve followed a predefined trajectory during period B0. Dry body weight was initially set as in period A and thereafter adjusted based on the information provided by the Hemocontrol refill indicator.
Study outcomes
The number of dialysis sessions affected by symptomatic IDH episodes, nursing interventions (Trendelenburg position, manual reduction of ultrafiltration rate, infusion of isotonic saline or hypertonic fluid, lowering of dialysate temperature), and the clinical symptoms of cramp, dizziness, and nausea not associated with IDH was counted. Pre- and post-dialysis systolic and diastolic BP, pre- and post-dialysis body weights, interdialytic weight gain, patient's subjective assessment of the degree of fatigue after dialysis (scale from 0 to 10; 0, not at all, 10, extremely) and recovery time from fatigue after dialysis (within minutes, when arriving home, at bed time, next morning, by next HD) were measured at the 4th and 8th week of period A and B1. A nurse measured blood pressure in the non-fistular arm on supine position after quiet resting of 5 min in accordance with contemporary recommendations. Post-HD BP was measured immediately after hemodialysis. Hemoglobin levels, blood chemistry, and dialysis adequacy data were collected.
Sample size
Assuming baseline frequency of treatments with IDH of 36% and expected 30% improvement in experimental period (odds ratio, 0.599) with α level of 0.025 (one-sided test) and 90% power, we determined that a sample size of 51 patients in each period was required. The sample size was calculated based on the correlation among observations in the same subject set to 0.5 and minimum 21 treatments recorded in each phase (allowing for 12% loss of treatments for evaluation). Considering approximate 15% dropout rate, we planned to recruit 60 patients.
Statistical analysis
Data are presented as mean±SD. Difference in IDH frequency between period A and period B1 was analyzed by paired t-test. Difference in the degree of fatigue after dialysis and recovery time from fatigue after dialysis between period A and period B1 was analyzed by Bowker test. The correlation between the reduction rate of IDH frequency and the demographic or clinical parameters in period A was analyzed by Pearson correlation analysis. Differences were considered statistically significant when the P value<0.05. The SAS system for Windows (Version 9.2) was used for all analyses.
Ethics statement
The local institutional review board of each individual center approved the study protocol. IRB number of the Catholic University of Korea, Seoul St. Mary's Hospital was XC11DSMP0055K. All patients enrolled in the study offered written informed consent. This study was registered with the International Standard Randomised Controlled Trial Number Registry (ISRCTN96130697).
RESULTS
Patient characteristics
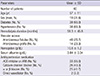
Seventy six patients were enrolled and 60 patients completed the study. The reasons for drop out were IDH incidence<25% in period A (n=8), transfer to other centers (n=4), high Hb levels (n=2), protocol violation (n=1), and consent withdrawal (n=1). The baseline characteristics were shown in Table 1. Anti-hypertensive medications and dialysis blood flow rate (261±44 mL/min) did not change in each patient.
Frequency of IDH and the number of nursing interventions
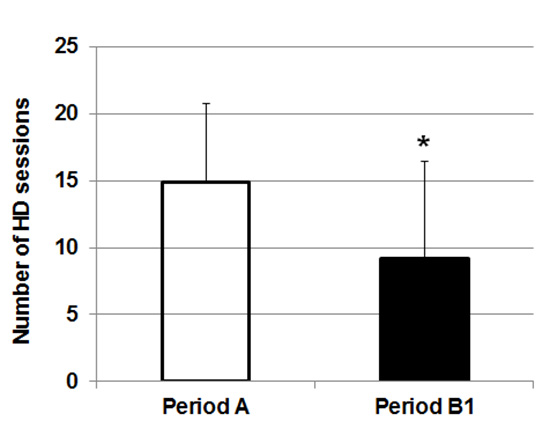
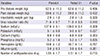
The number of sessions complicated by symptomatic IDH during 24 HD sessions was 14.9±5.8 sessions (62.1%) in period A and 9.2±7.2 sessions (38.4%) in period B1 with a decrease by 42.2% in period B1 (P<0.001) (Fig. 1A). The number of IDH-related nursing interventions in a session was also significantly less in period B1 (0.96±0.66 in period A vs 0.56±0.54 in period B1, P<0.001) (Fig. 1B). In addition, the number of IDH-related nursing interventions in an IDH occurred session was significantly less in period B1 (1.46±0.52 in period A vs 1.37±0.41 in period B1, P<0.001) (Fig. 1C). However, the number of sessions complicated by muscle cramp, dizziness or nausea without IDH during 24 HD sessions did not differ between two periods (0.52±1.75 in period A vs 0.52±1.55 in period B1).
Blood pressures
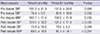
The mean pre-dialysis BP measured at the 8th week of each period did not differ between period A and period B1. However, the mean post-dialysis systolic and diastolic BP and MAP were significantly higher in period B1 than in period A (Table 2).
Degree of fatigue and recovery time from fatigue after dialysis
The patient's subjective assessment of the degree of fatigue after dialysis did not differ between period A (5.42±2.59 at 4th week, 5.42±2.47 at 8th week) and period B1 (4.80±2.33 at 4th week, 4.88±2.74 at 8th week). However, the more reduction of IDH frequency in period B1 was correlated with less degree of fatigue after dialysis (r=-0.33, P=0.009 at 4th week, r=-0.39, P=0.002 at 8th week). Furthermore, the recovery time from fatigue after dialysis (within minutes 10.2%, when arriving home 25.4%, at bed time 42.4%, next morning 22.0%, by next HD 0% in period A vs within minutes 23.7%, when arriving home 39.0%, at bed time 20.3%, next morning 13.6%, by next HD 3.4% in period B1) was significantly shorter in period B1 than in period A (P=0.048) (Fig. 2). The recovery time from fatigue after dialysis in period B1 was also negatively correlated with the reduction rate of IDH frequency (r=-0.36, P<0.001 at 8th week).
Body weight, dialysis adequacy and laboratory data
The mean pre- and post-dialysis body weight and interdialytic weight gain measured at the 8th week of each period did not differ between period A and period B1. The dialysis adequacy measured by urea reduction ratio, serum electrolytes, serum albumin levels, and hemoglobin levels did not differ between period A and period B1 (Table 3).
Reduction rate of IDH frequency
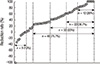
The reduction rate (%) of IDH frequency in period B1 showed wide variation. The reduction rate was ≥80% in 12 patients (20%), ≥60% in 22 patients (36.7%), ≥40% in 33 patients (55%), and ≥20% in 46 patients (76.7%). On the other hand, it was ≤0% in 9 patients (15%) (Fig. 3). Pearson correlation analysis revealed that the reduction rate of IDH frequency was positively correlated with the post-dialysis systolic and diastolic BP, and the pre- and post-dialysis body weight in period A, and was negatively correlated with the frequency of IDH and the difference between pre- and post-dialysis diastolic BP in period A (Fig. 4). On the other hand, it was not correlated with the age, HD duration, presence of diabetes, pre-dialysis BP, interdialytic weight gain, hemoglobin levels, serum albumin levels, and urea reduction ratio in period A. The reduction rate of IDH frequency did not differ between diabetic patients (median 44.0%) and non-diabetic patients (median 42.4%).
DISCUSSION
In this study, we found that compared with conventional HD, blood volume monitoring by HBS decreased the frequency of IDH (by a mean 42.2%) and the number of IDH-related nursing interventions, in addition to the faster recovery from fatigue after dialysis, in hypotension-prone HD patients. In Asian hypotension-prone HD patients, the reduction rate of IDH frequency induced by HBS was comparable to that observed in Western HD patients (30%-56%), although previous studies had small patient numbers, varying inclusion criteria, and different definitions of IDH. Consequently, these studies showed a wide variation in the baseline IDH frequency (7%-64%) before using HBS (16, 17, 19, 20, 21, 22, 23). We confirmed that HBS might be useful in Asian hypotension-prone HD patients. Our study also found that the number of IDH-related nursing interventions per session in period B1 decreased significantly, thereby reducing the burnout of HD nurses and improving patient compliance. Furthermore, HBS HD was associated with a significantly higher post-dialysis BP and less difference between the pre- and post-dialysis MAP, which was suggestive of improved hemodynamic stability, with no difference in interdialytic weight gain and actual body weight in comparison with conventional HD.
IDH results from a reduction of circulating blood volume and an impaired cardiovascular compensatory response due to the reduction in blood volume. Some reports showed that autonomic neuropathy was involved in the pathogenesis of IDH. In our study, 65% of patients had diabetes mellitus (DM), representing a larger diabetic population than those of previous studies. Despite the inclusion of a large number of DM patients, the response rate to HBS was comparable with that in previous reports. The prevalence of autonomic dysfunction is high in DM. However, previous studies showed that the prevalence of autonomic neuropathy was 20%-40% in pre-dialysis diabetic patients and 63% in non-diabetic HD patients (24, 25, 26). Taken together, these data suggest that it is not the diabetes itself, but the degree of autonomic neuropathy that might contribute to the reduction rate of IDH induced by HBS. Unfortunately, we did not assess the prevalence of autonomic neuropathy in our study.
Santoro et al. (17) reported that patients with an IDH episode frequency <25% during conventional HD responded less to HBS, and concluded that a greater frequency of IDH episodes during conventional HD results in a better response to HBS. However, in that study, the baseline rate of IDH in patients with an IDH episode frequency of <25% during conventional HD was very low, and patients with 25%-50% IDH episodes seemed to respond better to HBS than patients with an IDH episode frequency of >50%. In contrast, our study included patients with an IDH episode frequency of >25 and demonstrated that more frequent IDH during CBP HD results in less response to HBS. This might be due to severely impaired cardiovascular compensation caused by volume reduction in patients with more frequent IDH.
The Quality of life of IDH patients was assessed in three studies. One study found a 10% reduction in dialysis-related symptoms during the inter-dialysis period using blood volume-controlled HD compared with that using conventional HD (17). Another used the Kidney Disease and Quality of Life-Short Form (KDQOL-SF) questionnaire to show a significantly improved burden of kidney disease score in the hemocontrol group and a deteriorated score in the standard HD group (19). The third study found no difference in dialysis-related symptoms, as assessed by a questionnaire, between conventional HD and HBS HD (23). In our study, a greater reduction of IDH frequency by HBS was correlated with a lesser degree of fatigue and faster recovery from fatigue after dialysis. To determine whether HBS improves quality of life, further studies using validated tools are required.
The strengths of this study lay in the fact that this was the first multicenter prospective trial that assessed the efficacy of HBS in Asian hypotension-prone HD patients, and that it included a relatively large number of participants. This study also had some limitations. First, our crossover design could have influenced the subjective assessment of the degree of fatigue and recovery from fatigue after dialysis by the patients. Second, the dry weight was assessed by study physicians based on clinical evaluation. More objective results could have been obtained by using an objective method such as bioimpedance or echocardiography. Third, cardiovascular disease was investigated by history. The cardiac function could involve the frequency of IDH. Finally, we did not assess the degree of autonomic neuropathy, for example by performing autonomic function tests, in our patients. This assessment could have provided information on the predictive parameters for the response to HBS.
In conclusion, we found that the HBS might improve patient tolerability to HD by reducing the frequency of IDH and promoting faster recovery from fatigue after dialysis in hypotension-prone Asian HD patients.



 XML Download
XML Download