

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Right-sided infective endocarditis (RIE) is far less common than left-sided infective endocarditis (LIE) accounting for 5%-10% of all cases of infective endocarditis (IE) (1). In western countries, RIE occurs predominantly in intravenous drug users (IDUs) although patients with pacemakers, central venous catheters (CVC), and congenital heart disease (CHD) are at risk for RIE (2, 3). In previous studies, the proportion of IDUs among patients with RIE varied significantly from 46% to 86% (4, 5, 6).
Many studies have documented the clinical and echocardiographic features of RIE occurring in IDUs (2, 4, 5, 6, 7, 8, 9, 10, 11). RIE in IDUs has been reported to have a better prognosis than LIE in IDUs with an in-hospital mortality of 0% and 7%, respectively (2, 8). One of the studies reported that between 40% and 90% of IDUs with IE are HIV infected, and IDUs with IE and human immunodeficiency virus infection had a higher total mortality compared IDUs with IE and without HIV infection (11). Panidis et al. reported that 55% to 65% of RIE in non-drug users were caused by Streptococcus viridans, whereas Staphylococcus aureus was the predominant cause of RIE in drug users (12). Considering the difference in co-morbidity or etiology of IE between IDUs and non-drug users, clinical features and prognosis of RIE in non-drug users would be different from those of RIE in IDUs.
However, there are no studies on RIE in non-drug users without HIV infection. There are only case reports of tricuspid valve endocarditis or pulmonary valve endocarditis in non-drug users (12, 13, 14, 15, 16). Most of the knowledge regarding the surgical therapy for tricuspid valve endocarditis is also based on RIE in IDUs, and the experience with surgical intervention in non-addict patients is limited in Western countries (17). Korea has a very low prevalence of intravenous drug use, and most cases of RIE in Korea occur in non-drug users unlike in Western countries. Therefore, we conducted a retrospective study to analyze the clinical and echocardiographic characteristics of RIE in non-drug users.
MATERIALS AND METHODS
Patients
We performed a retrospective chart review of all cases diagnosed with IE over a 14-yr period from January 1995 to January 2009 at the Samsung Medical Center (Seoul, Korea), a tertiary university hospital. Cases were identified by all electronic discharge diagnoses of IE. Medical records, laboratory tests, and echocardiographic data of all the cases were reviewed. From the medical records, underlying medical disease, recent history of hospitalization, intravenous drug use including illicit drugs and medical drugs, and history of acupuncture were reviewed. If the patients had a history of intravenous illicit drug use on the records, we considered them as IDUs. The diagnoses of IE were retrospectively reassessed using the modified Duke criteria (2000). Finally, 345 cases, which satisfied the modified Duke criteria for a definite or possible IE diagnosis, were analyzed. According to the site of the detected vegetation, cases were divided into LIE or RIE. Among the 345 cases with IE, cases without definite vegetation or cases with vegetations in both sides of the heart on echocardiography were excluded from this analysis. Information pertaining to demographic characteristics, clinical, microbiological and echocardiographic features, outcome and complications was collected.
Echocardiography
All of the patients included in this study underwent transthoracic echocardiography (TTE). Transesophageal echocardiography (TEE) was also performed in about half of the patients. We reviewed all available echocardiographic studies at the time of diagnosis, and focused on the vegetation site, vegetation size, the presence of severe regurgitation of the involved valve, and complications such as abscess and perforation. The vegetative mass was measured in various planes. Vegetation size was measured by maximal length and width during freeze-frame analysis. Valvular regurgitation and its severity were graded by color Doppler imaging, using semiquantitative standard criteria. A perivalvular abscess was defined as a circular echo density, without flow in its interior.
Microbiology
Blood cultures were performed according to the hospital's standard guidelines, which recommend 3 culture sets from separate venipuncture sites when IE is suspected. However, in some cases, only 2 culture sets were obtained initially. Serological tests were not performed as part of the standard diagnostic procedure.
Definitions and analysis
RIE was defined as IE with vegetation in the right atrium (RA), tricuspid valve (TV), right ventricle (RV), or pulmonary valve (PV). LIE was defined as IE with vegetation in the left atrium (LA), mitral valve (MV), left ventricle (LV), or aortic valve (AV). Nosocomial IE was defined as IE associated with medical procedures performed in a hospital within the 8-week period before the onset of the disease, and/or IE occurring at more than 72 hr after admission. The underlying cardiac condition was classified as normal valve, congenital structural abnormality, or prosthetic valve, which was observed by echocardiography. Congenital structural abnormality included only uncorrected congenital heart disease (CHD) with structural abnormality, or corrected CHD with residual structural abnormality detected by echocardiography. Rheumatic heart disease or other abnormalities of native valves including degenerative changes were not categorized. Large vegetation was defined as vegetation equal to or larger than 2 cm in maximal length. Mural vegetation was defined as vegetation attached to sites other than valves, and it was mostly attached to the wall of one of the cardiac cavities. Embolic events included systemic embolism and pulmonary embolism. Only cases confirmed by imaging tests (computed tomography scan, magnetic resonance imaging, or echocardiography) were counted. In-hospital mortality was defined as death between admission and discharge, regardless of the cause of death. Cases with both RIE and LIE were excluded from the analysis, and IE cases without vegetation were also not included. In order to investigate the features of RIE in non-drug users, we compared each finding of RIE to that of LIE diagnosed using the same diagnostic criteria during the same study period.
Statistics
For comparisons in the distribution of continuous variables between RIE and LIE, Mann-Whitney U test was used; for comparisons of categorical variables, chi-square test was used and Fisher's exact test was used when the minimum expected count was less than 5. When the P value was less than 0.05, the difference was considered statistically significant. All analyses were performed with SPSS version 13.0 (SPSS Inc, Chicago, IL, USA).
RESULTS
Patients
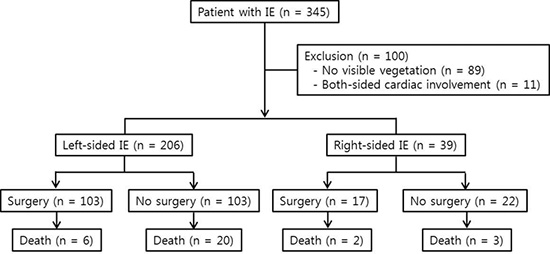
During the 14-yr study period, 345 cases were diagnosed with IE using the modified Duke criteria. Among these 345 cases, 89 cases without vegetation and 11 cases with vegetation in both sides of the heart were excluded from the analysis. Among the 245 finally included cases, 206 cases (84.1%) were classified as LIE and 39 cases (15.9%) were classified as RIE (Fig. 1).
Clinical characteristics
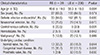
In our study population, there were no IDUs and no patients with HIV infection. The clinical characteristics of RIE compared with LIE are summarized in Table 1. In the RIE group, the mean age was significantly less than that in the LIE group (40.6±19.0 yr vs 50.3±18.0 yr, P=0.004). Sex distribution was not different between the two groups (male; 69.2% vs 64.6%, P=0.574). Cases with CVC (20.5% vs 3.9%, P=0.001) and cases with CHD (35.7% vs 13.1%, P<0.001) were more frequently found in the RIE group. Among the 15 RIE cases with CHD, ventricular septal defect (VSD) was the most common anomaly, and it was observed in 11 cases. Patent ductus arteriosus (PDA) was observed in 2 cases, atrial septal defect (ASD) in 1 case, and tetralogy of Fallot (TOF) in 1 case. IE occurring in normal valve was also more common in the RIE group (33.3% vs 18.9%, P=0.044). IE occurring in prosthetic valve was more common in the LIE group (2.6% vs 15.5%, P=0.030). Among the 13 cases of RIE in a normal valve, there were 6 cases with CVC. The frequency of the following variables was not statistically different between the RIE and LIE groups; definite IE by modified Duke criteria (84.6% vs 81.1%, P=0.600), nosocomial IE (25.6% vs 14.1%, P=0.070), cases on hemodialysis (5.1% vs 4.9%, P=0.942), and cases with malignancy (12.8% vs 12.1%, P=0.999).
Echocardiographic findings
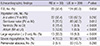
All of the patients included in this study underwent TTE, while TEE was performed in 22 cases (56.4%) of the RIE group and in 124 cases (60.2%) of the LIE group. The echocardiographic findings of two groups are shown in Table 2. In the RIE group, the TV was involved in 22 cases (56.4%), and 8 cases (20.5%) had vegetation on the PV. In the LIE group, the MV and AV were involved in 139 cases (67.5%) and 88 cases (42.7%), respectively. Mural vegetation was more frequently observed in the RIE group than in the LIE group (15.4% vs 0.5% in the ventricle, 12.8% vs 0.5% in the atrium, respectively). In the RIE group, all 6 cases with vegetation in the RV had VSD. Among the 5 cases with vegetation in the RA, 4 cases had an indwelling Hickman catheter. On comparing the vegetation size between the two groups, large vegetation (≥2 cm) was more frequently observed in the RIE group (33.3% vs 9.3%, P<0.001). Severe regurgitation was more common in the LIE group (48.1% vs 10.4%, P<0.001). The frequency of detection of perivalvular abscess was not different between the two groups.
Microbiology
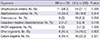
Blood culture data for both RIE and LIE cases are presented in Table 3. The most frequent microorganism causing RIE was S. aureus (n=13, 33.3%), followed by S. viridans (n=11, 28.2%). In the LIE group, S. viridans (n=64, 31.1%) was the most common causative bacteria and S. aureus (n=39, 18.9%) was the second most common causative bacteria. The distribution of causative microorganism was not significantly different between the RIE and LIE groups, except for S. aureus (33.3% vs 18.9%, respectively, P=0.044). Among the other organisms, fungal infection caused RIE in 2 cases (5.1%) and LIE in 4 cases (2.0%) (data were not shown in Table 3). Six cases (15.4%) in the RIE group and 46 cases (22.3%) in the LIE group had culture-negative IE.
Outcome
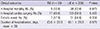
The short-term clinical outcomes in the two groups are shown in Table 4. Among the 39 cases in the RIE group, there were 5 deaths (12.8%) during hospitalization; and among the 206 cases in the LIE group, 26 patients (12.6%) died. In-hospital mortality rate was not different between the RIE and LIE groups (P=0.973). Seventeen cases (43.6%) in the RIE group and 103 cases (50.0%) in the LIE group underwent cardiac surgery during hospitalization, and no difference was observed between the two groups (P=0.463). Embolic events in the RIE and LIE groups were observed in 7 cases (17.9%) and 51 cases (24.8%), respectively (P=0.359). Duration of hospitalization was not different between the two groups (43.0±33.9 days vs 40.1±28.8 days, P=0.979). The characteristics of the five in-hospital mortality cases in the RIE group are described in Table 5. Mortality was directly associated with the following factors: uncontrolled sepsis (n=2), intracranial hemorrhage (n=1), pulmonary embolism (n=1), and massive hematemesis (n=1). Among these five in-hospital mortality cases, 2 cases had IE due to fungal etiology and 2 cases had large vegetation (≥2 cm).
DISCUSSION
Our study focused on investigating the clinical features of RIE in 39 non-drug users. In our series of RIE in non-IDUs, uncorrected CHD was the most frequent risk factor among the known risk factors of RIE, followed by CVC. In 15 cases of RIE with CHD, VSD was the most common anomaly. Previous reports on RIE occurring in patients with VSD showed that tricuspid valve involvement was the most common (15, 18). In our study population, the aortic valve (n=9) was most frequently involved followed by the tricuspid valve (n=8) in the total 27 IE cases with VSD. In addition, mural vegetation in the RV was observed in 4 patients with VSD. Isolated pulmonary valvular infective endocarditis (PVIE) is quite rare accounting for less than 1.5% to 2% of all cases of endocarditis (16). In the RIE group of the present study, the PV was involved in 8 cases; isolated PVIE was observed in 6 cases, and 2 cases had vegetations on the PV and in the RV. The underlying cardiac conditions in the 8 PVIE cases included PDA (n=2), VSD (n=2), ASD (n=1), TOF (n=1), and normal valve (n=2). This finding is similar to the reported autopsy analysis of nine cases of PVIE in non-addicts (19).
Anguita Sanchez et al. reported that the overall inpatient mortality of IE in non-injection drug users was 17%, and they showed that the mortality was significantly decreased in recent years (20). The in-hospital mortality in all cases of our study was 12.7%, which was almost similar to that in the other series of IE (20, 21, 22). Although two recent studies of IE that were performed in Korea showed a lower in-hospital morality of 3.0% and 7.0% as compared to that in our study, this difference seem to be due to different study populations (23, 24). Unlike these studies, our study included all IE patients who had various medical illnesses ranging from malignancy to multiple trauma. When we compared the in-hospital mortality between the first 7 yr and the next 7 yr during 14-yr study period, we observed a decrease in the in-hospital mortality from 17.7% to 10.2%. On the other hand, IE in IDUs has a relatively good prognosis. The mortality rate of IE in drug users ranges from 5% to 10%, depending on the series (4, 25, 26, 27). A study including 220 IDUs with IE reported a mortality rate of 5.2% from RIE in IDUs and a mortality rate of 11% from LIE in IDUs, thus showing an overall mortality rate of 6% from IE in IDUs (7). Thalme et al. found that treatment results for RIE in IDUs were good with no in-hospital mortality, no surgery, no relapses and no increase in long-term mortality (8). Unlike the prognosis of RIE in IDUs, the present study showed an in-hospital mortality of 12.8% in the RIE group, which was not better than that in the LIE group. In addition, the need for in-hospital cardiac surgery (43.6%) in the RIE group was not different from that in the LIE group. The high percentage of coexisting CHD with RIE may have resulted in a frequent need for cardiac surgery in the RIE group in this study.
S. aureus has been reported as the most common etiological pathogen, and it is observed in more than 50% of IE occurring in IDUs (9, 10, 25). Miró et al. showed that RIE in IDUs was casused by S. aureus in 77% (25). In this study also, S. aureus was the leading etiological agent of RIE (39% in positive culture), but the percentage was not as high as that in RIE occurring in IDUs. The distribution of causative organisms other than S. aureus and the proportion of negative culture were not significantly different between the RIE and LIE groups. When we analyzed the in-hospital mortality and in-hospital cardiac surgery for different etiologies, there were no statistically significant differences in either mortality or frequency of cardiac surgery (data not shown). A previous report documented that vegetation size larger than 2 cm and fungal etiology in RIE associated with in-hospital mortality (7). In our study, large vegetation (≥2 cm) was more commonly observed in the RIE group than in the LIE group. Among the five mortality cases in the RIE group, 2 cases had large vegetation, and in 2 cases, fungal infection was the etiology for RIE. However, because of the small number of patients, the prognostic significance of these findings remains unclear in this study.
Our study has several limitations. This study included a relatively small number of patients, especially in the RIE group. That is because RIE is far less common compared to LIE. In addition, the present study was a retrospective study. Although we could not identify any patients who use intravenous illicit drugs from the medical records, it may be possible that this information could have been missed during history taking. This problem is intrinsic to retrospective studies. However, there is a much smaller population that use intravenous illicit drugs in Korea compared to Western countries. Finally, the study subjects had various medical illness other than IE, which may make it difficult to compare the mortality in this study with that in another study.
In conclusion, in-hospital mortality and need for in-hospital cardiac surgery in RIE among non-drug users were not different from those in LIE; however, RIE in IDUs showed a favorable prognosis in previous reports. The most important risk factors for RIE in non-drug users are CHD and indwelling CVC. S. aureus is the most common etiological pathogen of RIE in non-drug users.


 XML Download
XML Download