

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Patent ductus arteriosus (PDA) is a common problem encountered in the early neonatal period, particularly in preterm infants. However, controversy regarding the treatment of PDA still exists. Of greatest concern is the treatment of PDA in extremely preterm infants "born at the limits of viability" because 1) the rate of spontaneous ductal closure is extremely low (1); 2) the response rate to pharmacologic treatment is very low as well (1, 2); and 3) they are prone to develop hemodynamically significant PDA with cardiopulmonary compromise (3). For these reasons, surgical ligation is frequently performed despite the surgical risk and complications. However, there is a paucity of data concerning the factors affecting neonatal outcomes after surgical ligation in extremely preterm infants. The purpose of this study was to investigate the prognostic factors associated with surgical ligation for PDA in infants born at 23 to 25 weeks of gestation.
MATERIALS AND METHODS
We retrospectively reviewed the medical records of all infants with a gestational age of 23-25 weeks. They were born and admitted to the neonatal intensive care unit (NICU) at Samsung Medical Center from January 2005 to December 2010.
Study population
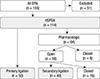
A flow diagram of the study population is shown in Fig. 1. A total of 165 extremely preterm infants was reviewed and 51 out of 165 infants were excluded because they showed 1) no visible PDA (n=21); 2) a very small PDA with a minimal shunt (PDA of no hemodynamic significance) on echocardiogram (n=7); or 3) congenital anomalies, birth asphyxia, or mortality within the first 48 hr (n=23).
A total of 114 infants had hemodynamically significant PDA. Of 114 infants, 50 infants were treated with primary surgical ligation because pharmacologic treatment was contraindicated. The remaining 64 infants were treated with either indomethacin (n=57) or ibuprofen (n=7). Of these 64 infants, 40 infants eventually underwent surgical ligation. Therefore, a total of 90 infants ultimately received surgical ligation (primarily or after pharmacologic treatment failure) and were included in this study.
Evaluation and management of PDA
A routine echocardiogram was performed on all infants within two weeks of birth as indicated by their clinical status. If the infants were confirmed to have left-to-right flow or bidirectional flow with a dominant left-to-right shunt through the PDA, and if there were any findings suggesting congestive heart failure, including tachycardia, hypotension, decreased urination, intolerable enteral feeding, cardiomegaly, etc., they were regarded to have hemodynamically significant PDA, and pharmacologic treatment was initiated as soon as possible (4). Indomethacin or ibuprofen was administered intravenously as a pharmacologic treatment. Prophylactic indomethacin was not used, i.e. all pharmacologic treatments were performed as a rescue therapy.
Surgical ligation was indicated if 1) one or two cycles of cyclooxygenase inhibitors failed to close the PDA, and the infants still had symptoms of congestive heart failure (n=40); or, 2) if there were any contraindications to pharmacologic treatment, including thrombocytopenia (platelet count<50,000/µL), renal dysfunction (urinary output of 0.5 mL/kg/h or less within 24 hr before surgery, plus serum creatinine≥2.0 mg/dL), or necrotizing enterocolitis (NEC)-like symptoms (abdominal distention, bluish abdominal color, or feeding intolerance with greenish gastric residue) (n=50).
An analysis of prognostic factors after surgical ligation
To analyze the prognostic factors associated with surgical ligation, infants were classified into two groups according to outcome: survivors with no major morbidity (N), and survivors with any type of major morbidity or non-survivors (M). Major morbidities included intraventricular hemorrhage (≥grade III), cystic periventricular leukomalacia, moderate-to-severe bronchopulmonary dysplasia, and necrotizing enterocolitis (≥ stage II). Intraventricular hemorrhage (IVH) was diagnosed by brain ultrasonography and graded by Papile's classification system (5). Bronchopulmonary dysplasia (BPD) was defined by the Jobe and Bancalari criteria of Ehrenkranz et al. (6). Necrotizing enterocolitis (NEC) was staged according to modified Bell's criteria (7) (Table 1).
Demographic characteristics, including gestational age, birth weight, small-for-gestational-age status, sex, Apgar score at 1 and 5 min, in vitro fertilization, pregnancy-induced hypertension, pathologically confirmed chorioamnionitis, and antenatal glucocorticoid administration, were compared between the two groups (Table 2). Gestational age was assessed by calculating from the first day of the mother's last menstrual period or by estimation from prenatal ultrasonography. Clinical characteristics associated with the evaluation or the management of PDA, including the use of pharmacologic treatment prior to surgery, mean postnatal age at the time of the first diagnosis of PDA, mean postnatal age at the time of surgical ligation, mean duration of exposure to PDA, and PDA size at the time of initial detection and surgical ligation were compared between the groups. Preoperative clinical conditions, including the incidence of pulmonary hemorrhage, hypotension, fraction of inspired oxygen (FiO2), and urine output within 24 hr prior to surgery were also compared between the groups. Hypotension was defined as when an infant's mean blood pressure measured less than the number of gestational age in weeks, with a need for inotropic support within 24 hr before surgery. Indications of ligation were also compared between the groups.
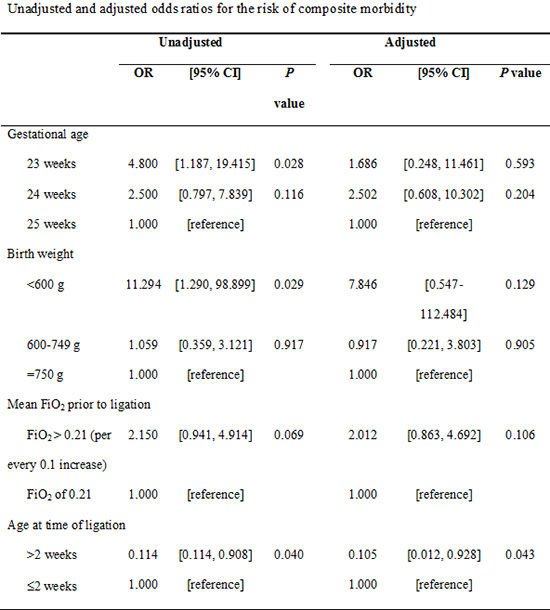
Unadjusted and adjusted analysis for the risk of composite morbidity
Possible prognostic factors derived from the preceding analysis were examined by unadjusted and adjusted logistic regression analysis. Odds ratios (OR) with 95% confidence intervals (95% CI) for the risk of composite morbidity were calculated and are shown in Table 3. A composite morbidity was defined as the occurrence of mortality or at least one of the major morbidities previously noted.
Statistical methods
The comparisons of demographic and clinical characteristics between the two groups were performed using chi-square tests or Fisher's exact tests for categorical variables and Student's t-test for continuous variables. A binary logistic regression was used for the unadjusted and adjusted analysis. All analyses were performed using Predictive Analytics SoftWare Statistics version 20.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
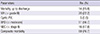
The outcomes after surgical ligation are shown in Table 1. Fourteen (15.6%) infants died and 69 (76.7%) infants had composite morbidity in this study. A comparison between N (n=21), and M (n=69) is presented in Table 2. The gestational ages were different between the groups, with the mean gestational age of M being lower than that of N (24.3±0.8 weeks in M vs 24.9±0.9 weeks in N). The mean birth weight of M was significantly lower than that of N (661±126 g in M and 731±85 g in N).
The rate of pharmacologic treatment in M was lower than that in N (39.1% in M vs 61.9% in N); however, it did not reach statistical significance. Notably, the timing of surgical ligation showed a significant difference between the groups. The mean postnatal age at the time of ligation in M was lower than that of N (11±8 days in M vs 17±12 in N). Additionally, mean FiO2 within the 24 hr prior to ligation was significantly higher in M compared to that of N (0.24±0.05 in N vs 0.30±0.12 in M). Otherwise, there was no difference between the groups with respect to prenatal and postnatal clinical characteristics.
Gestational age, birth weight, mean FiO2 prior to ligation, and the timing of surgical ligation were selected as possible prognostic factors and were included in further analysis (Table 3). In the unadjusted analysis, a gestational age of 23 weeks, a birth weight of less than 600 g, and mean FiO2 greater than 0.21 before ligation were each respectively associated with an increased risk of composite morbidity (OR of 4.800, 11.294, and 2.150, respectively), whereas delayed ligation (after 2 weeks) was associated with a decreased risk of composite morbidity (OR of 0.114 with 95% CI of 0.114-0.908). In the adjusted analysis, the increases in odds ratios at a gestational age of 23 weeks, a birth weight of less than 600 g, or mean FiO2 greater than 0.21 prior to ligation did not reach statistical significance. However, delayed ligation (after 2 weeks) still showed a significant decrease in the risk for composite morbidity over early ligation (within 2 weeks) (OR of 0.105 with 95% CI of 0.012-0.928) after adjusting for gestational age, birth weight, and mean FiO2 greater than 0.21 prior to ligation.
DISCUSSION
According to Koch et al., the spontaneous ductal closure rate and the complete response rate to pharmacologic treatment in infants with a gestational age of less than 25 weeks are approximately 2.5% and 9%, respectively (1). Our data showed them to be 5.8% and 12.5%, respectively, for infants with a gestational age of 23-25 weeks. Jhaveri et al. reported that 81% of infants born at 24-25 weeks gestation underwent surgical ligation, and our data showed that 79% of infants born at 23-25 weeks gestation required surgical ligation (3). Despite the high rate of surgical ligation in these infants, little is known about the prognostic factors associated with surgical ligation. The optimal timing of surgical ligation is also undetermined. Here, we found that delayed (>2 weeks) ligation was associated with a decreased risk for composite morbidity.
To prove that timing determines outcome, it is important to analyze the status of the PDA and any preoperative clinical conditions that might interfere with the outcome, because in early surgery, infants might be in a riskier condition that resulted in them receiving an earlier intervention. Despite the prevailing concerns of persistent opening of the ductus arteriosus, our results showed that delayed ligation and prolonged exposure to persistent PDA were not detrimental. Similarly, how early the PDA was diagnosed did not appear to matter, because the timing of the initial detection of PDA did not differ between the groups. The size of the PDA also did not appear to affect neonatal outcome. Preoperative cardiovascular and renal conditions indicated by the occurrence of pulmonary hemorrhage, hypotension, and oliguria showed no difference between the groups, and were also not likely to act as confounders. Of note, the FiO2 prior to surgery showed a significant difference between the groups. To exclude the possibility that preoperative respiratory conditions altered the results, univariate and multivariate analyses were performed. A FiO2 greater than 0.21 within 24 hr prior to ligation was associated with an increased risk of composite morbidity on univariate analysis (OR of 2.150 per every 0.1 increase of FiO2 with 95% CI of 0.941-4.914) with a nearly significant P value (P=0.069). However, the multivariate analysis revealed that it was not significant after controlling for gestational age, birth weight, and delayed ligation (OR of 2.012 per every 0.1 increase of FiO2 with 95% CI of 0.863-4.692, and P value of 0.106).
Ligation was indicated when pharmacologic treatment was contraindicated (primary ligation) or failed to close PDA (secondary ligation). As the timing of primary ligation was earlier than that of secondary ligation (10±6 days vs 16±9 days, P=0.002), contraindications could contribute to early ligation, leading to worse outcomes. Comparisons between the two groups with regard to contraindications of pharmacologic treatment showed that the incidence of renal dysfunction, thrombocytopenia, and NEC-like symptoms did not vary.
Because primary ligation was performed more frequently in M than in N with a nearly significant difference (P=0.082), it was necessary to determine whether pharmacologic treatment per se had a protective effect on composite morbidity. A univariate and multivariate analysis showed that the use of pharmacologic treatment did not alter the risk of composite morbidity (OR of 0.699 with 95% CI of 0.263-1.863 and OR of 0.672 with 95% CI of 0.205-2.202, respectively) (8).
According to the result of the multivariate analysis, delayed ligation is uniquely associated with increased risk of composite morbidity. It is, of course, inappropriate to assume that worse neonatal outcomes were entirely caused by early PDA ligation, given the limitations of this study that stem from its retrospective nature. This study simply highlights the necessity of a prospective study to clarify the causal relationship between the timing of ligation and neonatal morbidity.
A few previous studies have evaluated the optimal timing of surgical ligation in preterm infants. However, they have reported conflicting results (9, 10, 11, 12, 13). Moreover, these studies did not target extremely preterm infants at the limits of viability, although these infants undergo surgical ligation the most frequently and under the riskiest conditions. This was a single center study with a relatively large number of extremely preterm infants and also the first study to examine the prognostic factors associated with surgical ligation in such infants.
Because of the recent acknowledgement of the physiology of PDA and the adverse effects on various organ systems of treatment (14, 15, 16, 17), most current studies have focused on delayed treatment and a more conservative approach for preterm infants (18, 19, 20, 21). Considering the surgical complications and hemodynamic instability after ligation (22, 23, 24), we also believe that early aggressive intervention could be detrimental to these tiny infants. Although it would be difficult to reduce the rate of surgical intervention, our data suggest that it appears to be advantageous to avoid surgical ligation in the early, vulnerable period.
In conclusion, delayed surgical ligation of PDA is associated with decreased neonatal morbidity in extremely preterm infants born at 23-25 weeks of gestation. Further well-designed, randomized, controlled clinical studies and experimental studies will be needed to confirm the detrimental effects of surgical ligation in the early period of life and its precise pathophysiology in extremely preterm infants.


 XML Download
XML Download