

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Heart failure (HF) is a health problem worldwide, especially in developed countries, with a major cause of morbidity and mortality, leading to hospitalization (1, 2). Coronary artery disease including acute myocardial infarction (AMI) is the most common cause of HF, while HF is a common serious complication following AMI (3, 4).
In recent decades, introduction of new medical and interventional treatments, such as primary percutaneous revascularization, antiplatelet agents, renin-angiotensin-aldosterone system (RAAS) antagonists, statins, and hemodynamic support system such as intra-aortic balloon pulsation (IABP) and extracorporeal support system (ECS) have been reported to decrease the rate of HF development and in-hospital mortality of AMI patients (5, 6, 7, 8). However, some other studies could not find any significant decrease in trends, especially the incidence of HF after AMI (9, 10). Most studies about the trends in the AMI with HF (AMI-HF) were based on data in western countries. However, there are few data whether the improvements of AMI treatment have reduced the incidence or short term in-hospital mortality of HF in Asian countries (11). Accordingly, we sought to investigate temporal trends of AMI-HF in the clinical characteristics, treatment methods and in-hospital mortality in 1998 and 2008, respectively.
MATERIALS AND METHODS
Study design and population
We studied consecutive AMI patients who admitted in the five major university hospitals in Korea at two time points, 1998 and 2008. First, we used the discharge codes as coded by the International Classification of Disease, Tenth Revision, Clinical Modification (ICD-10-CM). AMI was defined as I21. We recognized a total of 1,785 patients with this AMI code. Eligible AMI patients for this study had any episodes of chest pain within two weeks of admission and a positive troponin test or electrocardiographic changes (ST-segment deviation ≥0.1 mV or pathologic Q wave). A total of 1,513 patients was selected for adopting these diagnostic criteria of AMI. The exclusion criteria were as follows: chest pain onset started two weeks prior to admission, underlying heart failure, estimated life expectancy of less than 12 months.
Baseline characteristics and definition of heart failure
The records of clinical variables were retrieved from patients' electronic medical record. Clinical variables included in the analysis were: age, gender, cigarette smoking, vital sign, family history of vascular disease, route of admission (emergent department, out-patient and in-hospital), co-existing conditions such as hypertension, diabetes mellitus, cerebrovascular accident (CVA), history of AMI one month prior to admission, and dyslipidemia. The location of infarction, treatment modality, additional mechanical treatment, total admission duration, discharge medication, and in-hospital death were also included.
Shock was defined as systolic pressure lower than 90 mmHg. Conservative care of AMI was defined as no reperfusion treatment such as thrombolysis, percutaneous coronary intervention (PCI), and coronary artery bypass graft (CABG). Diagnostic criteria of HF were defined as left ventricular ejection fraction (LVEF) by echocardiography less than 40% or dyspnea with congestion on radiograph.
Statistical analysis
Continuous variables were expressed as mean±standard deviation and are compared with the Student's t-test. Discrete variables were expressed as percentages and compared with the chi-square test or Fisher's exact test. A multivariate logistic regression analysis was performed in order to identify independent predictors for AMI with HF. Variables which were evaluated in the multivariate logistic regression analysis included using those with significant association (P<0.05) in univariate logistic regression analysis.
A propensity score matching analysis for the predicted probability of in-hospital mortality in each group was estimated with the use of logistic regression model fit with 18 clinically relevant factors. Age, gender, types of AMI (ST elevation MI), underlying comorbidities such as diabetes, hypertension, dyslipidemia, CVA, previous MI and family history, smoking status, systolic blood pressure, heart rate, revascularization methods (PCI and CABG) and adjuvant therapy (ventilator, intra-aortic balloon pump (IABP), inotropes and intensive care unit (ICU) care). We created a propensity score matched by attempting to match case patients and control patients (a 1:1 match). A nearest-neighbor-matching algorithm with a "greedy" heuristic (one that always implements the best immediate, or local, solution) was used to match patients on the demographic characteristics. All other analyses were 2-tailed, with clinical significance defined as values of P<0.05. All statistical analyses were done with Statistical Analysis Software package (SAS version 9.1, SAS Institute, Cary, NC, USA).
RESULTS
Characteristics of the study populations
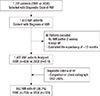
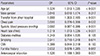
The flow chart was briefly presented to illustrate the selection process of study population (Fig. 1). Of 1,785 patients to have AMI coded with I21 (ICD-10-CM), we selected 1,513 subjects who satisfied the diagnostic criteria of AMI. We excluded 86 patients; and a total of 1,427 patients were finally selected in this study. There were 608 (42.6%) patients with AMI at 1998 and 819 (57.4%) at 2008. Baseline demographic and clinical characteristics are shown in Table 1. The patients of 2008 were older and had high proportion of male patients, hypertension, dyslipidemia, and previous AMI but lower prevalence of ST-elevation MI (STEMI) and received more revascularization treatments such as PCI and CABG and lower thrombolysis treatment and had shorter ICU care duration, compared to those in 1998.
Characteristics of AMI patients with or without HF
Considering the definition of HF as LVEF less than 40% or dyspnea with congestion on chest radiograph, a total of 552 (38.7%) patients had AMI with HF. The AMI patients with HF were more female gender, older, and had a higher incidence of transfer from other hospital, absence of chest pain at the initial presentation, lower systolic blood pressure, diabetes mellitus, smoking, CVA, family history and more anteroseptal MI, less received PCI, more received CABG, and longer admission and ICU care duration (Table 2). Multivariate logistic regression analysis showed that old age, transfer from other hospital, absence of chest pain, lower systolic blood pressure, increased heart rate and anteroseptal MI were independent predictors for AMI with HF (Table 3). In 1998, old age, transfer from other hospital, increased heart rate and anteroseptal MI were independent predictors for AMI-HF. In 2008, old age, transfer from other hospital, absence of chest pain, lower systolic blood pressure and anteroseptal MI were independently related to AMI-HF (Table 4). The AMI patients with HF in 2008 were older, had a higher prevalence of hypertension, previous AMI, and had more active treatment such as adjuvant therapy (e.g. ventilator, IABP, extracorporeal membrane oxygenation (ECMO) and inotropics), medical therapy (e.g. antiplatelets, beta blocker, RAAS antagonists, and statin) and lower systolic blood pressure compared to those in 1998. However, there was no significant difference for the incidence and overall in-hospital mortality of AMI-HF between the two time points (Table 5). To compare in-hospital mortality properly considering the severity of AMI-HF patients, propensity score matching analysis was done with 18 relevant clinical variables. However in-hospital mortality was not improved between the two time points irrespective of types of AMI and revascularization methods (Supplementary Table 1, 2, 3).
DISCUSSION
The major finding of this study is that despite major advances in the management of AMI, the incidence and in-hospital mortality of AMI-HF remained unchanged and still high. During the past few decades, advance of interventional treatment (e.g. IABP, DES) and induction of new medical treatments such as antiplatelet agents, beta-blocker, RAAS antagonists, and statins have markedly improved long term prognosis of patients with AMI (5, 6, 7, 12). In our study, while short term in-hospital mortality rate (3.3% vs 4.9%) was comparable to other previous studies but it was not decreased from 1998 to 2008. Considering the disparity in clinical severity between two time points in our study, increased hospital accessibility and advanced salvage treatments of high-risk AMI patients in recent time point may contribute to these unchanged trends.
Regarding HF complicating AMI, Hellermann et al. (13) showed that compared to 1979, there was a 28% reduction in the incidence of heart failure after AMI at 1994 in the Unites States. In Framingham Heart Study, compared with the period 1970 to 1979, the investigators observed higher risk of heart failure and lower risk of mortality rate in the period 1990 to 1999 (9). Consistently, in Canada, 5 yr rate of HF development increased by 25%, whereas 5 yr mortality rate after MI decreased by 28% (10). The incidence of AMI with HF did not change from 1998 to 2008 in our study, comparable to other studies (4). However, most epidemiologic studies about the trends in the incidence of HF after AMI have been conducted in Western countries. Recently, the striking differences in outcomes after AMI were observed in the different ethnic group studies. For instance, Chinese had higher short-term mortality, compared with South Asian and white patients (11). In our study, even after extensive propensity score matching analysis, in-hospital mortality was not improved between the two time points irrespective of types of AMI and revascularization methods. Rather, in hospital mortality of AMI-HF seems to be higher in 2008 than in 1998 (11.1% vs 6.4%, P=0.071), although it does not reach statistical significance. Higher referral rate from other hospital (41.7% in 2008 vs 36.1% in 1998, P=0.111), higher incidence of shock patients (11.1% in 2008 vs 5.7% in 1998, P=0.069) and higher incidence of previous MI (13.0% in 2008 vs 3.1% in 1998, P<0.001) might contribute to this finding. However, nationwide large prospective study with non-selected AMI patients would clarify the actual temporal trends of in-hospital mortality. In addition, future studies about the trends of HF following AMI in Asian region might be followed to confirm the disparities between western and East-Asian patients.
The studies to decipher the predictors for HF in AMI have been conducted. Najafi et al. (4) showed that age, current smoker, hypertension, diabetes, Q-wave and anterior wall MI were independent predictors of early-onset HF after MI. Ezekowitz et al. (10) reported that male gender, hypertension, diabetes, atrial fibrillation and CVA were associated with the risk for developing HF during hospitalization in MI. In HORIZONS-AMI trial, multivariate predictors of new-onset HF following PCI in STEMI were history of MI, LVEF, female and insulin-treated diabetes (14). In one study in Korea, old age, female gender, high serum creatinine and low LVEF were the predictors for long-term mortality in acute coronary syndrome patients with left ventricular systolic dysfunction (15). In consistent with these findings, we could find many HF risk factors in multivariate analysis (Table 3). Most of them were related to hemodynamic status (lower systolic blood pressure, increased heart rate) and co-morbid medical conditions (e.g. hypertension, diabetes, and CVA). AMI patients with HF in 2008 were older and, had a higher prevalence of hypertension, previous AMI, adjuvant therapy and lower systolic blood pressure than those in 1998. Considering these lines of findings, older age, transfer from other hospital, and lower systolic blood pressure at admission were important risk factors for HF development following AMI in Korea. Therefore more attentions and early treatments about concomitant HF should be paid in AMI patients with low systolic blood pressure and underlying medical diseases.
This study has several limitations. First, although we sought to analyze all consecutive AMI patients at two time periods, selection of patients was dependent on ICD codes of medical database without detailed clinical information such as laboratory and angiographic findings. Even though utilizing an administrative database with established quality control, the absence of validation of diagnosis and subsequent coding might be an important limitation. Though we excluded patients with underlying heart failure, there are possibilities that patient with asymptomatic LV dysfunction with no apparent heart failure symptom (NYHA II) could be enrolled as a patient with HF complicated AMI in this study. Second, because the data pertain only to one city and two times of year, this result may not be applicable to other nationwide patients. Third, the lack of long-term follow up data after discharge might underestimate overall HF incidence rates and prevent further analysis with long-term mortality of AMI-HF. Lastly but most importantly, we could not analyze the long-term outcome of AMI-HF patients. Therefore further prospective studies are required to reveal whether recent development of procedural managements and more evidence-based practice might improve midterm as well as long term survival after index admission of AMI-HF patients.
In conclusion, more evidence-based medical and advanced procedural managements were applied with patients with AMI in 2008 than in 1998, but there were no significant differences in the incidence of HF during hospitalization and in-hospital mortality following AMI between 1998 and 2008 in Korea.




 XML Download
XML Download