

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tumor necrosis factor-alpha (TNFα) inhibitors have demonstrated a significant effectiveness in patients with rheumatoid arthritis refractory to DMARDs (disease modifying anti-rheumatic drugs). In ankylosing spondylitis, any biologics except TNFα inhibitors have failed to show effect, so there are no alternatives (1, 2). Despite this dramatic effect, major concern about anti-TNFα therapy is the risk of developing serious infections, especially tuberculosis (TB). Since TNFα plays an essential role to form granuloma to contain Mycobacterium tuberculosis, inhibition of this effect results in vulnerability to active TB (3). Patients receiving TNFα inhibitors are at increased risk of developing both primary TB and reactivation of latent TB (LTB) (4-6). Therefore, LTB screening and chemoprophylaxis is mandatory before initiating TNFα inhibitors (7, 8).
Re-administration of TNFα inhibitors to patients who developed active TB during anti-TNFα therapy may deteriorate or reactivate TB. Thus, it is difficult to make a decision of the treatment regimen for patients with rheumatoid arthritis (RA) or ankylosing spondylitis (AS) flared after withdrawal of TNFα inhibitors due to active TB. American College of Rheumatology (ACR) guideline recommends that TNFα inhibitors could be resumed for RA management after completion of anti-TB treatment if clinically indicated, as evidence C (9). However, the safety and optimal time point of restarting TNFα inhibitors following TNFα-related TB have not been fully evaluated. In case of AS, there is no guideline about a re-introduction of anti-TNFα therapy following active TB. Only a few reports on re-adminstration of TNFα inhibitor after TB are available (10, 11).
This study was conducted to evaluate the safety of restarting anti-TNFα therapy in patients with TNFα-associated TB using medical records retrospectively. In addition, we determined the incidence and outcomes of TB related with anti-TNFα therapy.
MATERIALS AND METHODS
Study design and patients
We performed a retrospective study by using data of 1,012 patients from both the St. MAry RheumaToid Arthritis (SMART) registry and the St. MAry Ankylosing Spondylitis (SMAAS) registry to identify patients who developed active TB. The SMART registry was designed to prospectively collect all cases of RA patients receiving TNFα blockers from 1 January 2003 at Seoul St. Mary's Hospital, Seoul, Korea. The SMAAS registry recruited AS patients treated with anti-TNFα therapy from 1 January 2003 at Seoul St. Mary's Hospital. Between January 2003 and July 2013, the SMART registry enrolled 575 RA patients, the SMAAS registry recruited 437 AS patients. All patients fulfilled the 1987 (12) or 2010 American College of Rheumatology (ACR) criteria for RA (13) and the 1984 modified New York criteria (14) or The Assessment of Spondyloarthritis International Society criteria for AS (15). All study patients received TNFα inhibitors because AS or RA could not be controlled with DMARDs or NSAIDs. We obtained the results of tuberculin skin test (TST) or interferon-γ releasing assays (IGRA) to evaluate the incidence rate of LTB and checked whether they developed active TB or not.
We included patients with active TB during anti-TNFα therapy. Demographic and clinical data including sex, age, disease duration, history of TB, mean steroid dose, chest radiographs results, locations of TB lesions, treatment drugs and duration of TB, responses to anti-TB treatment were collected from medical records. We also investigated treatment drugs and clinical courses of underlying RA or AS in patients after a cessation of TNFα inhibitors due to active TB.
Diagnosis of LTB and active TB
TST and/or IGRA were checked for screening LTB. The TST was performed according to the Mantoux method, using 5 tuberculin units (TU) of purified protein derivative (PPD) standard or 2 TU of PPD RT-23 (Statens Serum Institut, Copenhagen, Denmark). A trained health-care worker recorded each patient's reaction to the TST at 48-72 hr after placement. A positive result was defined when the transverse diameter of the induration was ≥10 mm after 48-72 hr. QuantiFERON-TB Gold In-Tube test (QFT-GIT test; Cellestis Ltd., Carnegie, Australia) was used as IGRA test. The QFT-GIT was considered positive as ≥0.35 IU/mL. LTB was diagnosed when at least one of the two screening tests was positive without a radiological suggestion of active TB. Active TB were diagnosed by isolation of Mycobacterium tuberculosis from a clinical specimen or clinical decision depending on radiological or histological findings of TB with typical symptoms.
RESULTS
Incidence of active TB after initiating TNFα antagonists
Of total 1,012 patients, 15 patients were diagnosed with active TB during anti-TNFα therapy. Five cases were occurred in RA and 10 cases in AS. The incidence rates of active TB during anti-TNFα therapy were 220 per 100,000 person year (PYs) in RA and 609 per 100,000 PYs in AS. Before starting TNFα inhibitors 303 patients (29.9%) were diagnosed as LTB on screening tests. Chemoprophylaxis for LTB was given in 299 (98.7%) patients with LTB at least 1 month prior to initiation of TNFα inhibitors. Chemoprophylaxis regimen was the 9-month isoniazid (300 mg/day). Six (2%) of 299 patients developed active TB despite of chemoprophylaxis and were classified as prophylaxis failure.
Demographic and clinical characteristics of patients acquired active TB during anti-TNFα therapy
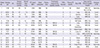
There were 11 male and 4 female patients with a median age of 44 (range 25-70) yr (Table 1). Patients who treated with adalimumab, infliximab or etanercept at the time of occurrence of TB were 9, 4, and 2, respectively. The median time from initiation of anti-TNFα therapy to development of TB was 19 months (range 2-65). Lung (66.6%) was the most common site of TB and there were 6 cases (40%) of extra-pulmonary TB. All patients had completely cured or improved active TB with combinations of anti-TB medications. The median treatment duration was 9 months (range 6-19). In two patients, levofloxacin was used instead of first line drugs due to adverse event or resistance to isoniazid.
All 5 patients with RA were classified as non-LTB due to negative TST and normal chest radiograph before starting anti-TNFα therapy. However, 4 of 5 patients developed active TB within 6 months of anti-TNFα therapy. All patients had denied any kind of contact with persons known or suspected to have active TB. They used steroids in addition to other immunosuppressants and three patients were taking over 10 mg of prednisolone at screening. No data were available on IGRA tests in these patients.
Among 10 patients with AS, 6 patients had performed chemoprophylaxis due to positive TST and 1 patient had a history of complete treatment of TB before anti-TNFα therapy. Two out of 6 patients had received chemoprophylaxis incompletely. Among 5 patients with old TB scar lesions on screening chest radiographs, 2 patients had underwent chemoprophylaxis due to positive TST and 3 patients had not due to negative TST.
Treatment of RA or AS in patients with active TB
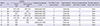
As a diagnosis of active TB was made, TNFα inhibitors were immediately stopped and switched to DMARDs or NSAIDs with/without corticosteroids. Eight (RA=3, AS=5) out of the 15 patients experienced disease flare after withdrawal of anti-TNFα therapy (Table 2). We resumed TNFα antagonists with the informed consents of patients. The median duration after the cessation of anti-TNFα therapy to re-introduction was 3 (range 2-7) months in RA and 12 (range 6-29) months in AS. Due to the differential risk of TB among TNFα inhibitors, 4 patients who had previously used adalimumab switched to use etanercept; and one patient in the infliximab group switched to use adalimumab. The rest 3 patients re-administered the previously received TNFα blocker because they wanted to use it. The re-introduction of anti-TNFα therapy resulted in prompt improvement of the disease activity in all patients. There was no recurrence of TB for 14 (median, range 5-39) months after re-introduction of TNFα antagonists. Three patients with RA and 1 patient with AS re-introduced to TNFα inhibitors even before the completion of anti-TB treatment did not experience any aggravation of TB. The rest of the patients showed a good response to DMARDs or NSAIDs previously failed to control the disease activity after development of active TB. They had been tolerable and remained in low disease activities for at least 8 up to 84 months (Table 3).
DISCUSSION
In this study, the estimated incidences of active TB in patients with anti-TNFα therapy was higher than general population (78.9 per 100,000 PYs) reported by World Health Organization (17). Because Republic of Korea is a TB endemic area, we compared our results with other recent study from Republic of Korea which reported that an incidence rate of TB was 771.6/100,000 PYs for those with RA and 600.2/100,000 (PYs) for those with AS (18). Our study showed lower incidence in RA, but similar incidence in AS. Despite vigorous screening for LTB and high chemoprophylaxis rate, incidences of active TB in RA or AS patients treated with TNFα inhibitors were increased than general population. This might be affected by underlying autoimmune disease by itself or false negative screening tests. We also considered whether isoniazid chemoprophylaxis was powerful enough to prevent reactivation of TB in patients with autoimmune diseases.
Nine of 15 patients who developed active TB had showed a negative TST before starting TNFα antagonists. In particular, 4 (45%) of 9 TST-negative patients developed active TB within 6 months of anti-TNFα initiation. This was considered to be reactivation of LTB in patients with false negative TST which could be affected by steroids and immunosuppression. Recently both TST and IGRA are recommended for screening LTB before anti-TNFα therapy to increase the detection rate of LTB. Kleinert et al. (19) reported that the prevalence of LTBI was 8.0% when defined as a positive TST, 7.9% as a positive IGRA and 11.1% as combining both tests. In this study, only one out of 9 patients was underwent both TST and IGRA for screening LTB. If both tests were used, it would increase the sensitivity of detecting LTBI.
Despite chemoprophylaxis for LTB, 6 patients developed active TB. They received chemoprophylaxis with isoniazid for 9 months. There was a possibility that some patients were infected with isoniazid-resistant strain. In recent years, attention has focused on three types of rifamycin-based short-course regimens for treatment of LTB (20). Guidelines from the Centers for Disease Control and Prevention recommended use of the 3-month isoniazid-rifamycin regimen as an equal alternative to the 9-month isoniazid regimen. It will increase compliance to prophylactic drug due to short duration with comparable efficacy.
Among 15 patients who developed active TB, 3 patients with RA (60%) and 5 patients with AS (50%) experienced flare after the discontinuation of anti-TNFα therapy. Other study reported that discontinuation of TNFα inhibitors resulted in disease flare in around 50% of patients with RA (21). And Brandt et al. (22) found that more than two-thirds of the patients with AS already had a relapse after 12 weeks and almost all patients had a relapse after 24 weeks of discontinuation of etanercept. In the case of infliximab, after 12 weeks of discontinuation 64% patients experienced a flare and after 52 weeks 97% patients had to be re-infused because of relapse (23). In our study, patients with AS had a lower flare rate compared with earlier reports and patients with RA were comparable.
Eight patients were recommended for anti-TNFα therapy at 8.5 months (median, range 2-29) after the initiation of anti-TB medication. Four of 8 patients who reinitiated TNFα inhibitors before completion of anti-TB treatment showed good response to anti-TB regimen and none of them experienced reactivation of TB. Matsumoto et al. (10) described a case that infliximab was resumed after 9 months of anti-TB medication in RA patient with peritoneal TB and no recurrence of TB for 10 months. In another report (11), infliximab was reintroduced for a patient with severe AS after 2 months of anti-TB treatment and no sign of TB recurrence was detected during 60 months. Aslanidis et al. (24) showed that 5 patients were diagnosed active TB infection among 180 RA patients and 3 of 5 patients recommended TNF α inhibitors at 6, 12, and 48 months after the initiation of anti-TB treatment. In consideration of these findings, re-initiation of anti-TNFα therapy could be effective and safe after at least 2 months of proper anti-TB medication.
Five of 8 patients were switched to other TNFα inhibitors after TB in pursuit to reduce the risk of worsening or recurrence of TB. Because almost of them were re-initiated TNFα antagonists before completion of anti-TB medication, we considered the difference of drug-specific incidence of TB. Tubach et al. (25) said that the risk of TB is higher for patients receiving anti-TNFα monoclonal antibodies therapy (infliximab or adalimumab) than for those receiving soluble TNFα receptor therapy (etanercept). This might have influence a good outcome and the absence of recurrence of TB.
Some limitations in our study should be noted. Because data collected from a retrospective cohort of a single center, number of cases with active TB and follow-up period might be not enough to prove the safety and the optimal time point for re-administration of TNFα inhibitors. Longer-term prospective studies with large sample size are needed to confirm our findings.
In conclusion, this study results suggests that re-administration of TNFα inhibitors could be safe and should be considered to control RA or AS flares for patients with anti-TNFα therapy-associated TB.

 XML Download
XML Download