

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Diastasis of the pubic symphysis is an uncommon peripartum complication that might result in a serious distress to the patient (1-3). The diastasis is considered to be related with hormonally induced ligamentous laxity (2, 4, 5). Clinical features and radiological findings of the diastasis have been well described in the literature (6-11). However, reported estimates of the frequency vary widely and the exact incidence of the diastasis is not known. In 1932, Reis et al. (12) first reported the separation of the symphysis pubis during labor. They estimated the incidence as 1 in 5,000 deliveries. In 1986, Taylor and Sonson (13) reported 11 cases of the diastasis. In their retrospective review, the incidence was 1 in 600 deliveries (13), which was 9-fold or more frequent than the incidence report of Reis et al. (12). Since then, several retrospective studies reported a similar incidence or much lower incidence (8, 14).
Previous studies speculated multiparity, forcep-assisted delivery, shoulder dystocia, maternal developmental dysplasia of the hip and prior pelvic trauma as predisposing factors for the diastasis. These studies were performed during the 1930s to 2000s and were not statistically supported (2-4, 12). Most patients improve symptomatically within the first few weeks, while some patients suffer persistent pain (4, 7, 8, 15). In some studies, the separation gap appeared to predict outcome (2), while it did not in other studies (11). Thus, the exact incidence and risk factors of diastasis are still remained uncertain.
In November 2003, medical staffs of the obstetric department and orthopedic department at our institution composed a committee to investigate the incidence and risk factors of the diastasis. All patients who had a peripartum pain at the symphysis pubis were consulted to the orthopaedic surgeons of the committee; and patients who were diagnosed as having a peripartum diastasis were registered and followed by the committee. In the current study we tried to determine the incidence and risk factors of pubic symphysis diastasis.
MATERIALS AND METHODS
Data base in EMR (electronic medical recording) of 4,266 women who delivered 4,695 babies at the obstetric department of Seoul National University Bundang hospital from January 2004 to December 2006 was reviewed with use of clinical data warehouse (CDW). Among them, 115 women (141 babies) with peripartum maternal death (1), still birth (99), or hysterectomy (15) were excluded. The remaining 4,151 women who delivered 4,554 babies were subjects of our study.
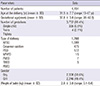
The mean age at the time of delivery was 31.5 yr (range, 15 to 47 yr). The mean gestational age was 37.8 weeks (range, 20 to 42.8 weeks). Three thousand seven hundred and fifty-two women delivered a single child, 395 women twins, and 4 women triplets. Two thousands two hundreds eighty-one women were primiparous, and 1,870 were multiparous. The type of delivery was normal full-term spontaneous delivery in 1,788 women, cesarean section in 1,689 women, preterm spontaneous delivery in 475, normal full-term vacuum extraction delivery in 172 women, preterm vacuum extraction delivery in 15, total breech extraction delivery in 7, and partial breech extraction delivery in 5. There were 2,079 male babies and 2,073 female babies with a mean body weight of 2.9 kg (range, 0.1 to 5.6 kg) (Table 1).
Among 21 women, who were consulted to orthopedic department due to a peripartum pubic pain, 11 women were diagnosed as having a peripartum diastasis of symphysis pubis. The diagnosis was made when the interpubic distance was widened by more than 10 mm at the narrowest point on pelvic anteroposterior radiograph (8, 16). Their mean age at the time of delivery was 34 yr (range, 29 to 38 yr) and the mean gestational age was 38.5 weeks (range, 35.2 to 40.3 weeks). Ten of the eleven patients were primigravida and one was multiparas. Four patients had twin gestation.
In two patients, pubic pain occurred during their gestation of 36+4 weeks and 38+5 weeks, respectively. The remaining nine patients had onset of pain after delivery.
The biparietal diameter of the newborn babies, which was measured in prepartum sonography, ranged 8.6 to 9.7 cm (mean, 9.22 cm). Their mean body weight was 2.92 kg (range, 2.4 kg to 3.6 kg). The mean diastatic width was 25.3 mm (range, 11.6-55.7 mm).
Ten patients delivered vaginally and one patient, who had a severe antepartum pain of the pubic symphysis, underwent caesarean section.
Three patients had a wide diastasis (>4 cm) according to the criteria of Kharrazi et al. (17) and the remaining eight patients had a diastasis of less than 4 cm. One of the three with a wide diastasis also had an anterior widening of the right sacroiliac joint. Two of the 3, who had a wide diastasis, suffered an intractable pain and were treated operatively with an open reduction and plate fixation. The remaining nine patients were treated conservatively with use of pelvic binders, lateral recumbancy, analgesics, and protected weight bearing.
The eleven women, who had the symphysis pubis diastasis, were categorized as patient group and 4,140 women, who had not, as control group. We calculated the incidence of symptomatic diastasis. To identify risk factors for the diastasis, we compared age, gestational age, number of gestations, parity, type of delivery, weight of the child, and gender of baby between the two groups.
The 11 diastatic patients were followed up at an interval of one week to one month after the diagnosis of the diastasis until the pain subsided and the radiographs were taken until the interpuic distance reduced or remained stationary.
The change of diastatic width was assessed on serial radiographs. The pelvis anteroposterior radiograph, which was taken immediately after the onset of pubic pain, was used as a baseline for the assessment.
Statistical analysis
Statistical analyses were performed using chi-square test or Fisher's exact test for categorical variables and Mann-Whitney test for numerical variables. All reported P values were two sided, and P value<0.05 was used to determine statistical significance.
Multivariate analysis was performed for variables, which had P values<0.10 in univairable analysis. Logistic regression was carried out to identify independent factors with regard to the diastasis. All statistical analyses were performed using SPSS (version 15.0, Chicago, IL, USA).
RESULTS
The incidence of peripartum pubic diastasis was 0.26% (11/4,151) in our study.
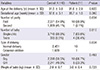
In univariate analysis, there were no significant differences between the diastasis patient group and postpartum patients without diastasis group with regard to age (P=0.887), gestational age (P=0.502), gender of baby (P=0.132), and body weight of baby (P=0.752). However, there were significant differences between the two groups with regard to parity (P=0.016), number of baby (P=0.003), and type of delivery (P=0.034) (Table 2). Adjusted multivariate analyses revealed that number of baby (OR, 9.20; 95% CI, 2.52-33.57, P=0.001), and type of delivery (OR, 12.6; 95% CI, 1.48-106.46, P=0.020) were significant factors for the diastasis.
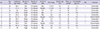
The diastatic patients were followed up for a mean of 22.1 months (range, 12 to 47 months). The interpubic distance of 9 patients, who were treated non-operatively, reduced to 0.7-1.3 cm over a period of 2 to 8 weeks and then plateaued (Fig. 1). Two operated patients had mild pubic pain at the latest follow-up (Fig. 2). Nine patients, who were treated conservatively, had gradual improvements of pain and ambulation over 2 to 6 months. However, 5 patients had symphysis pubis dysfunction; a persistent pain at the symphysis pubis during sexual intercourse (18). Two patients complained intermittent click at the symphysis pubis. These patients had a persistent instability of the symphysis pubis (Fig. 3, Table 3). Two patients with a wide diastasis showed a radiological finding of osteitis condensans ilii. However, they had no symptom on the sacroiliac joint at the latest follow-up.
DISCUSSION
Pelvic joint relaxation during pregnancy occurs by relaxin and progesterone, which enables normal vaginal delivery. The symphysis pubis diastasis which is a partial or complete rupture of the symphysis pubis may occur with associative factors including macrosomic fetus, small pelvis of mother, rapid progression of second stage of labor and rapid descent of presenting part, epidural anesthesia and pelvic trauma (8, 12, 14). The reported incidences of the diastasis vary widely from 1/300 to 1/30,000 in western countries (2, 3, 12, 19). The detection rate depends on physician's concern about this condition. The detection rate would be low if patients and physicians neglect a diastasis considering pubic pain as a transient unevenful symptom around labour. In our study, the incidence was 1/388, which was one of the highest among the reported incidences.
Our study was conducted in an East Asian institution. The high diastatic incidence of our study might be due to an ethnic difference and physicians' awareness with persistent concern about the diastasis during the study period.
Numerous factors including multiparity, macrosomia, cephalo-pelvic disproportion (CPD), previous trauma, abnormality due to congenital dysplasia, osteomalacia, chondromalacia, rickets, tuberculosis, rapid progression of second stage of labor and rapid descent of presenting part, and epidural anesthesia have been suggested as possible risk factors for the diastasis. However, these factors were speculative, which were not verified statistically. In our study, number of gestations appeared as the only risk factor.
Many authors have reported that functional recovery is excellent with conservative treatment (6, 7, 11). Most family physicians, obstetricians, and orthopedic surgeons, who can encounter diastatic patients in their own practices, consider their patients do not necessitate an operation and will recover with conservative management. However, an wide separation > 4 cm is usually associated with an skin-rupture of sacroiliac joint and instability of the pelvic ring (2), which necessitates a surgical intervention (17, 20). In our study, three patients had a wide separation; and two of them underwent open reduction and internal fixation due to unendurable pain. Although no patient had a gait difficulty, five patients (46%) suffered persistent symphysis pubis dysfunction and four patients had perceptual instability at the symphysis until the latest follow-up in our study.
This study has several limitations. First, we had a small number of patients; we identified only 11 diastatic cases over a period of 3 yr. A multicenter is warranted to precisely estimate the incidence and risk factors including labor time to incidences. Second, our study is based on a retrospective review of 4,140 non-diastatic women and a prospectively followed 11 diastatic patients. However, the data is reliable because our institution has adopted a comprehensive EMR system since May 2003 and achieved the stage 7 designation by HIMSS (Healthcare Information and Management Systems Society; Chicago, IL, USA) in 2010. Third, the incidence of cesarean section in this study is relatively high as forty-five percent of delivery. Our institution is a tertiary referral institution, which treats the high risk pregnancy including placeta previa or hypertensive disorder. Besides, cesarean section is frequently indicated in cases of previous cesarean section and breech presentation. Accordingly, our study lacks to exactly evaluate known risk factors of the diastasis. Fourth, asymtomatic diastasis, if present, has not been included in our study. However, we aimed to evaluate symptomatic diastasis. Finally, this study was performed at a single institution in East Asia, which cannot represent the ethnic difference and a caution should be exercised when making generalizations based on our results.
The incidence of symphysis pubis diastasis (1/385) in this study is higher than previously reported. The patients who are diagnosed with multiple gestations are at a risk of pubic symphysis separation and diastatic patients likely suffer persistent symphysis pubis dysfunction.



 XML Download
XML Download