

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Despite the great advances in the diagnosis and treatment of infective endocarditis (IE), it remains a disease with high inhospital mortality (16%-25%) and a high incidence of complications (1, 2, 3, 4, 5). In contrast to decreasing some of the other complications such as renal failure and uncontrolled intra-cardiac or metastatic infection with using antibiotics, embolic event is still a distressingly common complication of IE and this can occur even during administering appropriate therapy (6, 7). The incidence of clinically recognized embolism is known to 13% to 44% (6, 7). Adam et al. reported that cerebral infarction is a presenting sign of IE in 4% to 14% of all infective endocarditis (8).
All the patients who present with signs and symptoms of systemic arterial embolization should have IE considered as a possible cause (6, 7). Several studies have attempted to evaluate the predictors of embolic events and mortality. The reports have had conflicting results, vegetation > 10 cm in size, left-side valve infection and Staphylococcus aureus infection were suggested as the risk factors of embolic infarction (2, 9, 10, 11, 12, 13). Diabetes mellitus, Staphylococcus aureus infection and embolic events are known to be predictors of in-hospital mortality (3, 4, 5, 12). But there are few studies that have focused on the clinical influence of embolic event in IE and the predictors of in-hospital mortality in an Asian population.
The objective of this study was to investigate the clinical impacts of embolic event on IE and the predictors of in-hospital mortality. Determining the clinical effects of embolic event on IE and the predictors of in-hospital mortality may improve the management of this disease in hospitals.
MATERIALS AND METHODS
Patients and population
This retrospective study was performed at two teaching hospitals: Pusan National University Hospital, which is a 1,000-bed teaching hospital, between January 2003 and December 2010 and Pusan National University Yangsan hospital, which is a 700-bed teaching hospital, between January 2009 and December 2010. All the medical records were reviewed for the patients with infective endocarditis and who were over 18 yr of age. All the patients with infective endocarditis met the modified Duke's criteria (14) for definite IE or possible IE. The demographic data, the baseline characteristics and the outcomes were collected. The following data was recorded for each patient: age, gender, the underlying disease, the involved valves, a native valve versus a prosthetic valve, a community origin versus a nosocomial origin, the cardiac and extracardiac complications, the treatment given during hospitalization, the surgical requirements, the need for ICU admission, the echocardiographic findings, the total admission days and the in-hospital mortality.
Nosocomial IE was defined as an infection occurring more than 72 hr after admission to the hospital or the IE acquired in patients discharged from the hospital within 6 months before the onset of symptoms (15). Cardiac complication was defined as cardiac structural complication such as new onset of valvular functional abnormality, valvular abscess, valvular perforation and intracardiac abscess. Four to six blood cultures were obtained for all the patients.
Embolic event
We evaluated the radiologic/clinical evidence of embolism. The CT scans, MRI and chest radiographic findings were collected for the patients with signs or symptoms suggestive of an embolic event such as abdominal pain, chest discomfort, abrupt dyspnea and sudden neurologic or visual dysfunction. Renal and splenic embolisms were included if they were confirmed by radiographic imaging.
Statistical analyses
Statistical analyses were done using SPSS version 12.0 (SPSS Corp, Chicago, IL, USA). The descriptive analysis consisted of the median, mean and range of the various parameters. The differences between the embolic and nonembolic patients were compared using the chi-square test for the categorical variables, and the t-test or the rank-sum test was used for the numerical variables. Logistic regression analysis was performed to determine the predictors that were independently associated with in-hospital mortality. P values<0.05 were considered to be statistically significant.
RESULTS
Demographic features and the clinical outcomes
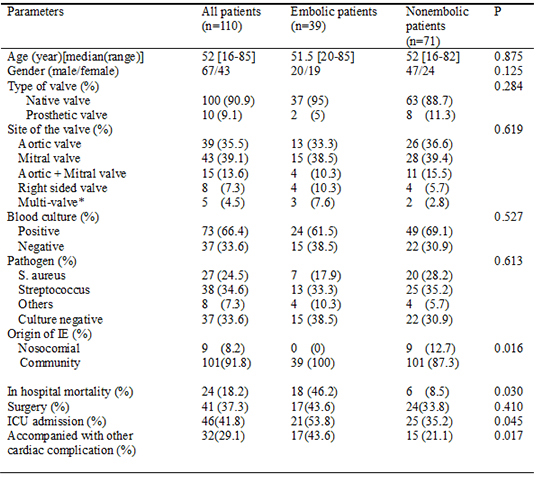
One hundred and ten patients who met the modified Duke's criteria for definite IE or possible IE (14) were analyzed. The median age was 52 yr (16-85 yr). Sixty seven patients (60.9%) were men and forty three patients (39.1%) were women. Most patients had native valve IE (n=100, 90.9%) and a community origin of IE (n=101, 91.8%). The mitral valve was the predominant infected valve (n=43, 39.1%) followed by the aortic valve (n=39, 35.5%). Eight patients with right-sided valve IE (7.3%) and five patients with multi-valve IE (4.5%) were observed. The most frequent causative organisms were Streptococci in 38 patients (34.6%), followed by Staphylococci in 27 patients (24.5%) and other organisms in 8 patients (7.3%), and these included 2 patients with Psuedomonas aeruginosa, 2 patients with Candida, 2 patients with Enterococcus, 1 patient with E. coli and 1 patient with gram-negative rods (not identified). Thirty-seven patients (33.6%) had culture negative endocarditis. Fifty-seven patients (51.8%) had underlying disease. Previous heart disease (n=37, 33.6%; 17 patients with valvular heart disease, 14 patients with congenital heart disease, 3 patients with heart failure, 1 patient with a prosthetic valve and 2 patients with coronary heart disease) was the most common underlying disease. The mean of total admission days was 36.1 days (range, 3-125 days) and 46 patients were admitted to the ICU. Surgery was performed on 41 patients (37.3%). Heart failure was main cause of surgical intervention (n=18, 43.9%) and median day of surgery was 4 admission days (range, 1-7). Failure of medical treatment is secondary cause of surgical intervention (n=12, 39.3%). In group of medical failure, 7 persistent bacteremia (>7 days) and 5 increasing vegetation and re-embolism during treatment were observed and median operation day was 12 admission days (range, 7-18). Large vegetation and high mobile vegetation were third cause of surgical intervention for prevention of embolism (n=6, 14.6%) and median surgery day was 5 admission days (range, 2-9). Three ventricular septum defect repairs (7.3%) and 2 permanent pacemaker insertion (4.9%) were undertaken.
Embolic events
Embolic events occur in 39 of 110 patients (35.5%). The brain (n=18, 38.5%) was main site of embolic infarction. Other sites included the spleen (n=12, 30.8%), the lung (n=11, 28.2%), the kidney (n=9, 23.1%), the liver (n=1, 2.6%) and main vessels (n=1, 2.6%). Multi-site embolic infarctions were observed in 19 patients (48.7%). Embolic events were recognized at the time of hospital admission in 30 of 39 patients with embolic events (76.9%) and other 9 patients (23%) were recognized during hospital management due to new clinical symptom. There were no significant differences in the demographic characteristics (age, gender, underlying disease, the involved valve site, causative organism, the type of infected valve and the positivity of blood culture) between the patients with and without embolism. But nosocomial IE was observed only in the patients without embolism (0% vs. 12.7%, respectively, P=0.016).
For the clinical outcome, the group of patients with embolism showed higher in-hospital mortality (46.2% vs. 8.5%, respectively, P=0.03), more frequent ICU admission (53.8% vs. 35.2%, respectively, P=0.045) and more accompanying other cardiac complication (43.6% vs. 21.1%, respectively, P=0.017). Table 2 shows clinical influence of embolic infarction in the patients with infective endocarditis.
In-hospital mortality
The in-hospital mortality rate was 18.2%. The leading causes of death were sepsis (n=8, 33.3%) and heart failure (n=5, 20.8%) and these were followed by brain complications (n=4, 16.7%), multi-organ failure (n=3, 12.5%), sudden death (n=3, 12.5%) and hospital acquired pneumonia (n=1, 4.2%). The causes of death in group of patients with embolism were surgery related infection and sepsis (n=6, 33.3%) and heart failure (n=4, 22.2%) and followed by brain complications (n=3, 16.7%: 2 brain hemorrhage: 1 massive brain infarction), multi-organ failure (n=2, 11.1%), sudden death (n=2, 11.1%) and hospital acquired pneumonia (n=1, 7.6%). In embolic group, there were no significant differences in in-hospital mortality between the patients with embolic event during management and the patients with embolism at the time of admission (55.5% vs. 43.4%, respectively, P=0.23). On the multiple logistic regression analysis of the predictors of in hospital mortality, age (RR, 1.079; 95% CI, 1.036-1.123, P=0.001), embolic event (RR, 3.510; 95% CI, 1.271-9.69, P=0.015) and staphylococcal infection (RR, 5.098; 95% CI, 1.308-18.508, P=0.023) were independently associated with in-hospital mortality (Tables 3, 4).
DISCUSSION
In this study, embolic events occurred in 35.5% of the patients with IE, and this was similar to that of the previous studies (30%-44%) (6, 7, 15, 16, 17). Contrary to several other studies (2, 9, 10, 11, 12, 13), there was no significant difference of the demographic characteristics (age, gender, underlying disease, the involved valve site, the causative organism, the type of infected valve and positivity of blood culture) between the embolic and non-embolic groups in this study.
Staphylococcus infection shows no difference between the embolic and non-embolic groups, but there was an independent association of Staphylococcus infection with in-hospital mortality in our study. In some earlier studies, Staphylococcus infection has been associated with both higher rates of complications and mortality in patients with IE (4, 11, 18), whereas other reports did not find any association between embolism and the causative microorganism (7, 21). The high rate of culture negative cases (33.6%) in this study could have affected interpreting the results about the causative organism. Previously receiving antibiotics is known to be the main cause of culture negative endocarditis (19, 20). In this study, out of 37 culture negative patients, 22 patients (59.5%) were referred from other hospitals under antibiotic treatment.
We evaluated the clinical impacts of embolism. The group of patients with embolism showed higher in-hospital mortality (46.2% vs. 8.5% respectively, P=0.03), more frequent ICU admission (53.8% vs. 35.2%, respectively, P=0.045) and a higher tendency to be accompanied with other cardiac complications (43.6% vs. 21.1%, respectively, P=0.017) as compared to the patients without embolism. Chu et al. (4) reported embolic events were closely related with surgery and mortality. Even though statistically significant differences were not observed, more patients of the embolic group received surgery (43.6% vs. 33.8%, respectively, P=0.410) in this study.
The in-hospital mortality rate was 18.2%, which was similar to those of other studies (3, 4, 5, 9, 18). Age, embolic events and Staphylococcus infection showed independent associations with in-hospital mortality in this study (Table 4). As for the predictors of mortality, several clinical variables have been investigated in previous studies, including age (22), Staphylococcus infection (4, 11, 18), prosthetic valve IE (2) and embolic events (2, 4, 9, 12, 13). Other studies have shown different results: Chu et al. (4) reported male gender, diabetes mellitus and the APACHE II score were independent predictors of mortality, and Hasbun et al. (5) reported comorbidity, an abnormal mental status, moderate to severe congestive heart failure and medical therapy without an operation were also independent predictors of mortality. Thuny et al. (9) showed a vegetation length >15 mm as a predictor of mortality. We could not find any correlation between the underlying diseases, including heart failure, diabetes or surgery, and the in-hospital mortality. Higher in-hospital mortality in the patients with a cardiac complications were observed, but there was no statistically significance. In the Asian population, Nomura et al. (23) reported "at least one complication" was a risk factor of mid-term mortality in 62 patients of a single center retrospective cohort. However there have been few studies on the predictors of mortality and the impact of embolism. Recognition of these predictors of in-hospital mortality and the impact of embolism can be expected to improve the risk stratification and allow for more intensive treatment of patient with IE.
This study has several limitations. First, the study was performed in two referral, large teaching hospitals. This is might have caused a selection bias, including a high culture negative rate and relatively faster operations, and it could have affected the evaluation of the predictors of in-hospital mortality. Second, the data on the vegetation size was not prospectively collected, so we could not evaluate the correlation between the vegetation size and the in-hospital mortality or embolism. Third, the study evaluated embolism on the basis of radiologic and clinical evidence. So clinically silent embolism may be not included in this study. Finally, this study may be affected by all of the limitations of the study's retrospective design. Therefore, further prospective large multi-centered studies are required to provide more accurate results in Asian populations.

 XML Download
XML Download