

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gastric cancer is one of the most common cancers worldwide. Although its global incidence is decreasing for several decades, it still constitutes one of the leading causes of cancer-related death worldwide (1). In Korea it is the most common cancer among males and third most common among females. Recently activated screening have lowered the mean age of its diagnosis. However its peak incidence still occurs in the seventh decade of life. The incidence of gastric cancer is expected to increase, owing to the extended life-spans of the general population.
Despite the large proportion of the elderly among gastric cancer patients, many clinical oncologists are reluctant to apply standard treatment to their elderly patients, being afraid of the potential risk of complications. Furthermore, there are no specific guidelines for this age group because of limited published data concerning gastric cancer in elderly patients. However, several recent studies have shown that gastric cancer in elderly patients has specific characteristics compared to that in young ones and that the age itself does not influence complications related to surgery (2). Also it has been suggested that young patients with gastric cancer show poorer prognosis (3). On the meanwhile, others reported that old age is related to poor prognosis (4). There are still no consensus about the features and surgical feasibility of the gastric cancer in the elderly.
The aim of this study was to evaluate whether gastric cancer in elderly patients has different characteristics from those in young patients and to investigate if standard surgical treatment strategy is suitable for this group of patients.
MATERIALS AND METHODS
Subjects
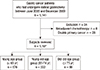
A total of 1141 patients underwent radical gastrectomy for gastric cancer between June 2005 and December 2009 at Seoul National University Bundang Hospital, a tertiary referral center. Radical gastrectomy was indicated when there were no evidences of either distant metastases or major vascular invasion. Patients with performance status 4 were not indicated. Patients with performance status 2 or 3 were allocated as the surgeons' decisions. Among them, 8 were excluded because of neoadjuvant chemotherapy and 26 were excluded for having double primary cancers. Therefore medical records of 1,107 patients were reviewed retrospectively. For analysis, patients who had endoscopic resections or incomplete resections were not enrolled.
Measures
Overall, the following variables were analyzed; age (<65, 65-74, or ≥75 yr), sex, type of chief complaint (no symptom, epigastric pain, dyspepsia, hematochezia, melena, hematemesis, or others), level of CEA and CA19-9, comorbidity (hypertension, diabetes mellitus, respiratory diseases, heart diseases, neurologic diseases, liver diseases, renal disease, or others), postoperative complication (surgery-related complication or disease-related complication), location of the tumor (upper, middle, or lower third of the stomach), TNM stage, Lauren classification (intestinal, diffuse, or unclassified), WHO classification (well differentiated adenocarcinoma, moderately differentiated adenocarcinoma, poorly differentiated adenocarcinoma, signet ring cell carcinoma, or mucinous adenocarcinoma), stromal reaction (absent, desmoplasia, neutrophils, eosinophils, lymphocytes, plasma cells, mucin production, histiocytes, or multinucleated giant cells), status of Helicobacter pylori, p53 overexpression, microsatellite status (microsatellite stable, microsatellite instability-low, or microsatellite instability-high), and combined synchronous gastric cancer. CEA level of 5 µg/L or less and CA 19-9 of 27 U/mL or less were considered to be normal. Overexpression of p53 was defined as expression rate greater than 50%. Synchronous cancers were defined as multiple cancers found in separate places in the stomach at the same time. When there were synchronous cancers, we took the deepest lesion for analysis of pathologic features. We chose the largest one when the choice was between lesions with the same depths of invasion.
Data analysis
All subjects were classified into the following three groups; young age group (<65 yr), young-old age group (65-74 yr), and old-old age group (≥75 yr). For staging, we adapted the seventh TNM staging system of American Joint Committee on Cancer Classification
(AJCC).
Statistical analysis
To evaluate differences among the three groups we performed the chi-square test for categorical variables and ANOVA for continuous variables. P values less than 0.05 were considered significant. All the analyses were performed with the Statistical Package for the Social Sciences, version 18.0 for Windows (SPSS, Chicago, IL, USA).
RESULTS
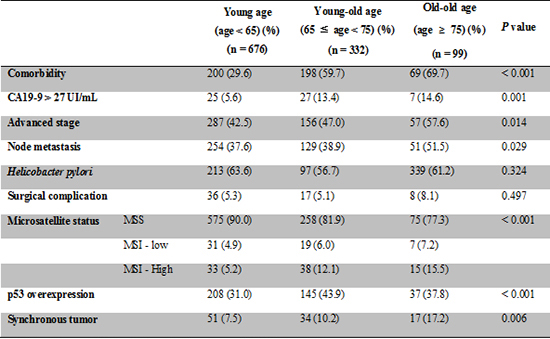
Among a total of 1,107 subjects, young, young-old, and old-old age group accounted for 61.1%, 30.0%, and 8.9%, respectively (Fig. 1). Mean age of the young age group was 51.8 yr, while that of the young-old and old-old age groups were 69.2 and 78.2 yr, each (Table 1). Male proportion did not show any differences among the three groups. There were more symptomatic patients among the old-old age group than the other groups (54.2%, 58.9%, and 73.2%; P<0.001). Screening abnormality was the most common chief complaint in all three groups with relatively low rate in the old-old age group (45.8%, 41.1%, and 26.8%; P=0.001), followed by epigastric pain, dyspepsia which was significantly more common in the old-old age group (15.6%, 19.9%, and 24.7%; P=0.045), melena, hematemesis, and hematochezia. Analysis of the tumor markers prior to the gastrectomy showed higher frequency of elevated levels of CA 19-9 in the young-old and old-old age groups (5.6%, 13.4%, and 14.6%; P=0.001). Overall comorbidities were more prevalent in the young-old and old-old age groups (29.6%, 59.6%, and 69.7%; P<0.001). Specifically, hypertension was the most common comorbidity in all three groups (18.9%, 42.5%, and 49.5%; P<0.001), followed by diabetes mellitus (8.3%, 17.2%, and 23.2%; P<0.001), heart diseases (1.6%, 7.2%, and 12.1%; P<0.001), neurologic diseases (1.8%, 3.6%, and 14.1%; P<0.001), respiratory diseases (0.6%, 4.8%, and 3.0%; P<0.001), liver diseases (1.0%, 1.8%, and 1.0%; P=0.572), and renal diseases (0.1%, 1.2%, and 4.0%; P<0.001). All these comorbidities except for liver diseases were more common in the young-old and old-old age groups. Rates of surgery-related complications such as wound problem, peritonitis, gastric perforation, incisional hernia, ileus, bleeding, pneumonia, atelectasis, etc. showed no differences between the three groups (6.1%, 6.0%, and 12.1%; P=0.067). Two patients in the old-old age group died from postoperative peritonitis. Other than surgery-related complications, there were 3 cases of disease-related complications such as acute stroke and acute kidney injury, of which 2 occurred in the young-old age group and 1 occurred in the old-old age group. Among the elderly patients including the young-old and old-old age groups, those with comorbidity did not have significantly higher rate of surgery-related complications compared to those without comorbidity (7.5% vs. 7.3%; P=0.947).
Lesions were most frequently located in the lower third of the stomach in all three groups (Table 2). Elderly patients had more advanced diseases with muscular invasion (42.5%, 47.0%, and 57.6%; P=0.014). Also node metastasis was more prevalent among the old-old age group with statistical significance (37.6%, 38.9%, and 51.5%; P=0.029). Using AJCC 7th TNM staging system, there were no significant differences among the three groups (P=0.122).
Regarding Lauren classification, there were more lesions of intestinal type in the young-old and old-old age groups (40.7%, 58.7%, and 56.6%; P<0.001), whereas diffuse type of lesions were more frequent in the young age group (54.3%, 33.4%, and 34.3%; P<0.001) (Table 3). In terms of WHO classification, the young-old and old-old patients more frequently had well differentiated (8.0%, 13.9%, and 13.1%; P=0.009) or moderately differentiated adenocarcinoma (29.6%, 44.0%, and 44.4%; P<0.001). Meanwhile poorly differentiated adenocarcinoma (40.5%, 29.8%, and 37.4%; P=0.004) and signet ring cell carcinoma (18.9%, 10.2%, and 5.1%; P<0.001) were more common among the young age group. With regards to stromal reaction, desmoplasia was more frequent in the young age group (19.3%, 12.4%, and 14.1%; P=0.018).
There were no significant differences in H. pylori status among the three groups (63.6%, 56.7%, and 61.2%; P=0.324) (Table 4). Overexpression of p53 (31.0%, 43.9%, and 37.8; P<0.001) was more commonly found in the young-old and old-old patients, however the old-old age group showed lower rate of overexpression than the young-old age group. Microsatellite instability (P<0.001) was more frequently detected in the young-old and old-old patients. Also young-old and old-old patients had more synchronous tumors (7.5%, 10.2%, and 17.2%; P=0.006).
DISCUSSION
Gastric cancer is considered to be a disease of the aged. Therefore its incidence is expected to rise with the increase of aging population. Some have reported that gastric cancer in the elderly patients does not have poor prognosis (5). However, standard treatment strategy for gastric cancer in elderly patients is yet to be established and whether this group has different characteristics from the others is still controversial. Therefore this study was designed to evaluate whether gastric cancer in elderly patients has different features from that in young patients and to investigate if standard surgical treatment strategy is suitable for this group of patients.
In our study, there were no significant differences in male proportion between the three age groups. However compared with the young age group, the young-old and old-old group had more male patients. It was the same as several previous studies (5, 6, 7). Although the reason for this is not clear, it is suspected to be because of the more frequent and prolonged exposure to carcinogen in the elderly male patients (8).
As for symptoms, there were more symptomatic patients among the old-old age group in this study. This might be because that the elderly people undergo screening tests less compared with young people. The fact that more elderly patients were diagnosed at advanced stages supports this assumption. Among the symptoms, nonspecific dyspepsia was significantly more frequent among the old-old age group. Therefore more surveillance should be recommended to the elderly population.
The elderly patients more frequently showed elevated levels of CA 19-9. Even though CA 19-9 is known to be ineffective in screening, they could be more useful for gastric cancer screening among elderly patients.
Comorbidities only except for liver diseases were more frequent among the elderly patients, and which was statistically significant. Also there were more patients among the elderly patients who had multiple comorbidities. However, despite the more prevalent comorbidities, postoperative surgery-related complications were not significantly frequent among the elderly patients. Furthermore, there were no differences in the rate of surgery-related complications between those with and without comorbidity among the elderly patients. Therefore radical surgery is thought to be applied to gastric cancer in elderly patients without significant risk of complications. This finding is similar to the result of a previous study about ovarian cancer, which revealed that extensive upper abdominal surgery is feasible in elderly patients (9). However considering that elderly patients have more risk of disease-related complications and larger rate of comorbidities, the decision for whether to do surgery for those with serious comorbidities should be considerate. Also, as growing number of cancer patients are surviving and increasing attention is paid to their continued health problems (10), non-cancer comorbidities of elderly gastric cancer patients should be managed more consciously.
Previous studies have reported that age itself is closely related to low survival rate in gastric cancer (11, 12). Delayed diagnosis and more advanced stage of gastric cancer in elderly patients are assumed to be possible causes of the low survival rate. However radical resection has been revealed to be associated with higher survival rate even in elderly patients (13). These findings also suggest the necessity of radical surgery for the elderly patients.
In terms of location, there were no significant differences among the three age groups. However there were tendency of more lesions located in the lower third of the stomach in the elderly patients. This finding is consistent with other reports (5, 14). As lesions in this part of the stomach are easier to resect and have better prognosis, radical resection would be feasible and tolerable in the elderly. Furthermore, as lesions in this area are more feasible to detect during endoscopic search, screening tests in aged population would have better efficacy.
In regard to the depth of invasion, there were more advanced diseases among the elderly patients. Also, node metastasis was more commonly found among the elderly patients. Considering the well-known fact that extent of wall penetration is an independent prognostic factor in gastric cancer, this might be related to less favorable prognosis of the gastric cancer in elderly patients. However, pathologic findings showed more favorable features among the elderly patients, such as intestinal type and well to moderately differentiated adenocarcinoma. Intestinal type is known to have better prognosis, whilst diffuse type has been reported to have worse prognosis with deeper invasion (15). From this finding, it can be inferred that gastric cancer in elderly patients generally have less aggressive features but are tend to be diagnosed at more advanced stages because of less frequent screening and more vague symptoms among the elderly people. Unlike in Western countries, however, D2 lymphadenetomy is the standard for surgery in advanced gastric cancer in Korea (16), therefore there are more chances that surgical treatment would be beneficial to elderly patients.
We applied the staging systems of the 7th AJCC to see if there are any differences in stage distribution between the different age groups. In this study, no differences in stages were found between the three groups. As only resectable cases were enrolled in our study, the majority of subjects were at stage I. Therefore it is difficult to say that the distribution of stages in elderly patients is not different from that of the others. As for microsatellite status, there were more lesions with microsatellite instability among the elderly group compared with the others. Considering that microsatellite instability correlates with good prognosis in gastric cancer (17), this is another evidence supporting that gastric cancer in elderly patients has less aggressive pathologic features.
This study revealed no differences in H. pylori status between the various age groups. The elderly patients, however, more frequently had intestinal type of adenocarcinoma which is known to be closely related to chronic H. pylori infection, therefore it is that they might have past H. pylori infection. As H. pylori incidence is gradually decreasing, true rate of H. pylori infection including past infection would be higher in the elderly group. In a recent study, H. pylori eradication could reverse the inflammatory change and levels of angiogenic factors dramatically (18). Therefore active eradication therapy for aged people is needed.
Interestingly, in this study, the elderly patients had a tendency towards p53 overexpression, which is known to be related to vascular invasion, as well as carcinogenesis (19). Other than this profile, gastric cancer in elderly patients showed pathologic features related to favorable prognosis. This may mean that the elderly have more chances to develop p53 mutation in aging process, which in turn causes susceptibility to gastric cancer.
Similar to several previous studies (20, 21, 22), we clarified more synchronous cancers develop among the aged. This might be related to the high incidence of intestinal type gastric cancer in this age group. It has been suggested that intestinal type of gastric cancer may be followed by multifocal carcinogenesis in the stomach with underlying atrophic gastritis (20). Therefore more scrupulous examination during endoscopy for the aged is recommended.
Consequently, as surgery in the elderly has no more risk than that in the young patients, we recommend looking favorably upon radical surgery for elderly patients with operable gastric cancers. However, considering the more advanced diseases and synchronous tumors among the elderly, the extent of surgery should be tailored accordingly.
There are several limitations to this study. One is that this is a retrospective research. However it still has an advantage of large number of subjects. Another limitation is that we only enrolled the patients who had undergone curative radical resection. Thus inoperable cases with advanced stages or early stage lesions which were treated endoscopically were not analyzed. Surgery might have been avoided more frequently because of severe comorbidity in elderly patients. However, even among the elderly patients, surgery-related complications were not increased by their comorbidities. For a more concrete analysis, a study including all the patients diagnosed with gastric cancer regardless of treatment modality is needed. Another limitation is that this study is not dealing with the data of survival. This should be investigated after enough follow-up duration is obtained.
From this study, it is suggested that despite the more comorbidities, radical surgery can be safely applied to elderly patients without significant risk of complications. Therefore, elderly patients with operable gastric cancer should be candidates for radical resections and more surveillance is needed for this age group. However, considering the more advanced diseases and synchronous tumors among the aged, care should be taken while deciding the extent of surgery in old patients.




 XML Download
XML Download