

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma is a common chronic illness that affects more than 300 million people worldwide. The incidence and prevalence of asthma is increasing in most countries (1). Asthma is a chronic inflammatory disease with a repetitive relapse and remission course (2); thus, it is very important to achieve and maintain effective control as a treatment goal. Despite scientific advances in diagnosis and treatment during the past two decades, asthma accounts for considerable healthcare costs and loss of work productivity.
An association between asthma and depression has increasingly been recognized (3, 4). Epidemiological studies have shown that depression is more common in patients with asthma compared to the general population (5). Moreover, asthma is associated with increased rates of depression (6). Although the causal relationship between asthma and depression is not fully understood, depression affects the outcome of asthma management. Depression may influence behavioral factors such as treatment compliance, self monitoring, and the management of environmental triggers, which may result in poor asthma control. Evidence suggests that depression is associated with morbidities due to asthma, including lower quality of life, asthma symptoms, and the requirement of more healthcares (7, 8). Therefore, detecting depression in patients with asthma could be of great importance for asthma management. However, there is little information on the risk factors for depression or their impact on asthma control in adult patients with asthma. The clinical characteristics of depression between non-elderly and elderly patients with asthma are thought to be different, considering that depression is generally associated with demographic, behavioral, and health-related factors.
In the present study, we examined the prevalence of and risk factors for depression in Korean adults with persistent asthma, with a focus on the potential differences between elderly and non-elderly patients.
MATERIALS AND METHODS
Study subjects
Patients with persistent asthma were prospectively recruited from five allergy and asthma centers covering diverse areas of Korea from September 2011 and October 2012. The patients were eligible if they were ≥20 yr of age, had physician-diagnosed asthma based on the Global Initiative for National Asthma (GINA) Guidelines at least 6 months prior to enrollment (9), had a predicted forced expiratory volume in 1 s (FEV1) ≥60%, and had been treated with inhaled corticosteroid (ICS), ICS plus a long-acting β2-agonist, or a leukotriene modifier during the previous 4 weeks. Patients who were not fluent in Korean were excluded. Individuals were also excluded if they had a diagnosis of another chronic respiratory illness including chronic obstructive lung disease or a chronic severe illness affecting quality of life (e.g., heart failure, chronic renal failure, or stroke). Patients were approached during their visit and informed of the study. If they agreed to participate, they were enrolled and classified into the non-elderly group (20-64 yr of age) or the elderly group (≥65 yr of age).
Demographic characteristics and pulmonary function testing
The patients were asked a series of sociodemographic questions, including age, sex, education level, employment status, type of family living arrangement, economic status, smoking status, and alcohol use. Economic status was classified as low, middle, high income, and patients were required to define their economic status according to their judgement. Body mass index (BMI) was checked and classified as follows: normal or underweight (BMI <25 kg/m2), overweight (25-29.99 kg/m2), and obese (≥30 kg/m2). Medical history, including disease duration, medication status, and co-morbidities were self-reported and verified by medical chart review. All patients underwent pulmonary function testing by trained pulmonary technicians according to American Thoracic Society recommendations.
Assessment of depression
Depression was assessed using the Patient Health Questionnaire-9 (PHQ-9), which has been translated and standardized for use in the Korean population (10). The PHQ-9 is a nine-item depression module taken from the full PHQ. It is a self-reported questionnaire that assesses each of the nine criteria in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition for clinical depression on a scale from 0 (not at all) to 3 (nearly every day). Its sensitivity and specificity are high compared to other depression questionnaires (11). A higher PHQ-9 score represents more severe depressive symptoms, where a score ≥10 is considered the standard cutoff indicating depression.
Asthma control and quality of life
The asthma control test (ACT), which was translated into Korean, was performed to evaluate asthma control. The ACT is an excellent tool for assessing control of asthma, although it is based on subjective measures. An ACT score ≥20 has been defined as well-controlled asthma (12).
Asthma-related quality of life was assessed with the Asthma-Specific Quality of Life (AQOL) questionnaire. The AQOL is an easy, validated tool with good psychometric properties for assessing the quality of life of patients with asthma (13). It includes 30 items representing six overall domains of physical and social activities, difficulties related to cough, emotional status, symptoms related to breathing, uncertain future, and environmental distress. Each item is scored on a five-point scale. A higher AQOL score is correlated with better quality of life.
Statistical analysis
All analyses were performed using SPSS 16.0 software (SPSS Inc., Chicago, IL, USA). Values are means±standard deviation (SD) or frequencies (%). The Student's t-test and chi-square test were used to determine differences between the two groups. Logistic regression analysis was used to calculate odds ratio for factors predicting depression in patients with asthma. Pearson's correlation test was used to evaluate the association between depression and ACT and AQOL score. A P value<0.05 was considered significant.
Ethical statement
This study protocol was reviewed and approved by the institutional review boards of Ajou University Hospital (IRB Number, MED-SUR-11-193), Kosin University Gospel Hospital (IRB Number, 11-100), Hallym University Sacred Heart Hospital (IRB Number, 2011-I066), and Dong-A University Hospital (IRB Number, 11-131). Written informed consent was obtained from each patient.
RESULTS
Patient characteristics
A total of 202 patients (mean age, 56.3 yr; range, 20-84 yr; 81 [40.1%] men) were enrolled, and their baseline characteristics are summarized in Table 1. The rates of non-smokers, ex-smokers, and current smokers were 61.9%, 22.3%, and 13.4%, respectively. The mean predicted percent FEV1 on the pulmonary function test was 88.8%. About 90% of the patients had been treated with maintenance inhalers, and almost all patients reported good medication compliance (98%). The ACT and AQOL scores were 19.9±3.6 and 94.2±23.2, respectively.
Prevalence and determinants of depression in adult patients with persistent asthma
The PHQ-9 score was 4.9±4.8 in all subjects, and the prevalence of depression based on the PHQ-9 was 16.8%. The prevalence of depression was 18.9% in the non-elderly group and 13.3% in the elderly group. Table 2 shows the clinical characteristics of the patients with asthma and depression. Patients with asthma and depression were younger (P=0.003), reported a lower economic status (P=0.048), had a shorter duration of asthma diagnosis (P=0.005), and a lower score on the ACT and AQOL (P<0.001) compared to subjects without depression. No significant differences in gender, smoking history, presence of co-morbidities, or lung function were observed between the groups. In addition, no difference was found for asthma medication compliance.
In the non-elderly groups, subjects with depression were significantly younger (40.4±12.8 vs. 49.4±12.1 yr) and had shorter disease duration (4.6±4.7 vs. 9.3±19.2 yr) than those without depression (Table 2). Depression tended to be more prevalent in unemployed subjects and those with lower economic status (P=0.052 and P=0.066, respectively). Subjects with depression in the elderly group had significantly higher BMIs (overweight status; 80% vs. 46%) and were current smokers (30% vs. 3.1%) compared to those without depression. No significant differences in age, economic status, or disease duration were observed. However, ACT and AQOL scores were significantly lower in subjects with depression.
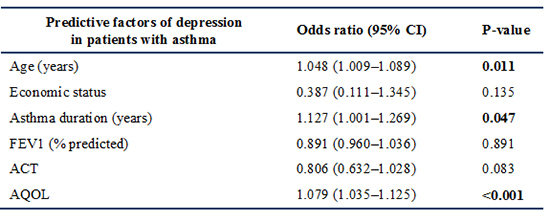
We performed a multivariate logistic analysis to identify factors related to an increased risk for clinical depression. The results revealed that age, asthma duration, and AQOL score were independently associated with the development of depression in adult patients with persistent asthma (Table 3).
Association between depression and asthma outcomes
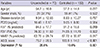
All subjects were classified into asthma-controlled or uncontrolled groups based on ACT score, and their clinical features are summarized in Table 4. No significant differences were observed between the groups in terms of age, sex, or disease duration. However, lung function and AQOL scores were significantly lower in the uncontrolled group than in the controlled group (P=0.019 and P<0.001, respectively). Depression was significantly more prevalent in the uncontrolled than in the controlled group (28.6% vs. 10.6%, P=0.001).
Patients with asthma and depression had significantly lower ACT and AQOL scores, indicating poor asthma outcome, and this result was similar when the participants were classified into non-elderly and elderly groups (Table 2). No significant difference was found in compliance with asthma controller medications and lung function according to depression status.
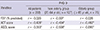
Next, we evaluated the relationships among PHQ-9 score, lung function, and ACT and AQOL scores. No significant correlation was observed between the PHQ-9 score and FEV1 values, but PHQ-9 score was inversely correlated with ACT and AQOL scores (r=-0.428, r=-0.553, respectively) (Table 5).
DISCUSSION
An increased prevalence of depression in patients with asthma is expected due to the impact of asthma on quality of life. Previous studies have reported that the prevalence of depression in patients with asthma is 7.5%-41% in other countries, which is greater than that in the general population (3, 14), although significant between-study variability has been observed in these studies. Moreover, it has reported the prevalence of depression in COPD patients was 23.8% in our country, and depression was more common in elderly patients than in young patients (15). However, a little information is available about depression in Korean adult asthma patients. In the present study, we conducted a survey targeting adult patients with persistent asthma using the PHQ-9 questionnaire, and confirmed a high prevalence (16.8%) of depression. This is the first investigation to compare differences in depression between non-elderly and elderly adult patients with asthma. Previous studies have reported that elderly patients with asthma are more likely to suffer from depression (16, 17), despite the fact that depression is less prevalent among older adults than among younger adults in the general population (3). We found a lower prevalence of depression in elderly than in non-elderly adults (13.3% vs. 18.9%), which may have been because we excluded elderly patients with chronic severe illnesses that affect quality of life.
There are reported that various sociodemographic characteristics
such as gender, marital status, education, income were risk factors for depression in general population (3, 18). However, our results demonstrate that younger age, shorter disease duration, and AQOL score were risk factors for depression among patients with persistent asthma. Besides, depression was more commonly found in subjects with lower economic status and ACT score among the patients with persistent asthma, although this was not statistically significant in the multivariate logistic analysis. These findings suggest that lower economic status and ACT score can be considered as modifiable factors for development of depression in asthmatic patients. The risk factors for depression were different between the non-elderly and elderly groups; younger age and shorter disease duration were significantly associated with depression in the non-elderly group, whereas high BMI and current smoking status were significantly associated with depression in the elderly group. Many studies suggest that depression causes obesity and smoking, in cases of asthmatic patients, it is known that obesity and smoking status are related to uncontrolled asthma (19). Besides, there has been a recent study demonstrating that obesity increases the risk of depression (20). Therefore, we suggest that higher BMI and current smoking status can be considered as risk factors for depression in elderly asthma patients, not in the non-elderly asthma patients. Our results suggest that clinicians should pay particular attention to factors that contribute to depression when managing adult patients with chronic asthma.
The impact of depression in patients with asthma is important, as it can be related to asthma control and prognosis. Studies have reported that depression is associated with poor asthma outcome, based on diverse outcome measures such as asthma-related quality of life, asthma-related health costs, need for additional therapy, and medication compliance (7, 8, 21, 22). Our results show that depression is significantly more prevalent in patients with uncontrolled asthma than in patients with controlled asthma, and that patients with asthma and depression have low ACT and AQOL scores. Moreover, the more severe the depressive symptoms, the poorer the asthma control and quality of life in both non-elderly and elderly adult subjects with asthma, although we did not evaluate asthma severity. A few reports have suggested that depression may be related to asthma severity with a higher prevalence in patients with severe and difficult-to-treat asthma (23, 24, 25). However, this association was not found in another study (26), indicating that the evidence does not strongly support a relationship between asthma severity and depression. In addition, several studies have reported significant correlations between depressive symptoms and poor lung function (27, 28). However, we did not find a correlation between these factors. Medication compliance was also not related to depression, although depression has been associated with non-compliance with medication and asthma treatment as well as a variety of medical conditions (29, 30, 31). We may not have detected this association because we only enrolled patients on regular treatment. Our findings confirm that depression can impact asthma control status and quality of life in both elderly and non-elderly groups.
The mechanism for impact of depression on asthma is less clear. However, it is thought that depression may induce behavior resulting in worse asthma outcome (32). Other studies have suggested that psychological and emotional factors may have biological effects on immunological and hormonal functions. Although the mechanisms are not fully understood, psychological stress can affect the release of cortisol and the expression of inflammatory mediators, which would increase airway inflammation (33).
There are several limitations to this study. The major limitation is that depression was assessed by questionnaire and not by a physician, although the PHQ-9 questionnaire is an excellent depression-screening method. Second, this was a cross-sectional analysis so causation or temporality of the association between depression and adult asthma could not be determined. Third, our findings may have underestimated the actual occurrence of depression because patients experiencing depression may be less likely to participate in a study. In addition, this study has a limitation in evaluating the overall prevalence as it was carried out only in five allergy and asthma centers based on university hospital setting, although they were covering diverse areas of our country.
In conclusion, we confirmed that depression is strongly associated with poor asthma control and quality of life, with a high prevalence of depression in Korean adult patients with persistent asthma. Our results present the differences of risk factors for depression between non-elderly and elderly patients with asthma, which provide important clues that can be used to target modifiable factors that contribute to depression and make asthma worse in adult patients with persistent asthma.
 XML Download
XML Download