

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Type 2 diabetes (T2DM) is a complex disorder due to the combination of genetic and environmental factors (diet, physical activity, etc.). Impaired pancreatic β-cell function and insulin resistance (IR) in muscle, fat and liver are pathogenic for T2DM (1). Recent genetic and genome-wide association studies have identified the DNA sequence differences (polymorphisms/mutations) in genes that encode proteins contributing to either insulin biosynthesis/secretion or insulin action. Among the genes related to T2DM, ectoenzyme nucleotide pyrophosphate phosphodiesterase 1 (ENPP1), also known as plasma cell membrane glycoprotein 1 (PC-1), reduces insulin signaling by inhibiting the insulin receptor tyrosine kinase activity (2). Costanzo et al. (3) showed that the human Q121 allele has more potent inhibitory effects on IR autophosphorylation than the K121 allele in vitro. Abate et al. (4) and Wang et al. (5) reported the association of the Q121 allele with diabetes in South-Asian and Han Chinese. However, no association was reported in the other Asians including Korean (6), Japanese (7) and Chinese (8). There are a few epidemiologic data associating ENPP1 K121Q polymorphism with the risk of T2DM among Koreans.
The discipline of nutrigenomics focuses on the effects of ingested nutrients and other food components on gene expression and gene regulation (9). The epidemic rise in the incidence of T2DM has fuelled research on the complex interplay between genes and environmental factors in the pathogenesis of the hyperglycemic diabetic state (10). Nutrigenomics has emerged as a multidisciplinary field that focuses on studying the interactions.
Lifestyle intervention can prevent or delay T2DM (11). Stefan et al. (12) investigated the influence of different polymorphisms on the effects of lifestyle intervention. In another study, the Q allele in the ENPP1 gene was significantly associated with an impaired increase in OGTT-derived insulin sensitivity after lifestyle intervention (13). Also, Moore et al. (14) reported that the K121Q polymorphism modulated the efficacy of lifestyle intervention on the incidence of T2DM. Therefore, Weyrich et al. (15) suggested that general methodological approaches to study gene-lifestyle interactions are needed. However, recent studies addressing the role of ENPP1 K121Q on lifestyle intervention have not demonstrated gene-by-dietary change-by-weight loss interaction.
In this study, we aimed to demonstrate a potential interaction between K121Q and web-based lifestyle intervention, and to verify whether the improvement of glucose metabolism observed after weight loss was associated with ENPP1 K121Q polymorphism.
MATERIALS AND METHODS
Subjects and study design
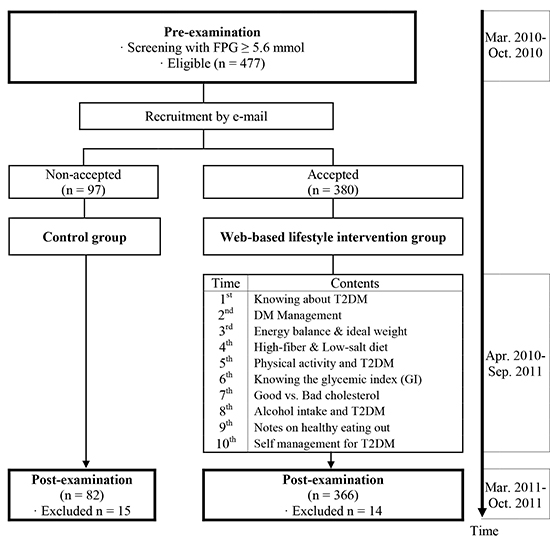
Flow chart of Participants during the study is shown in Fig. 1. The subjects were recruited from industrial male workers by screening members of the T2DM risk group who participated in annual regular health check-ups in 2010. Exclusion criteria were previously diagnosed T2DM, dyslipidemia, hypertension, cardiovascular disease, and any therapy known to affect glucose and lipid metabolism at basal screening. A total of 477 eligible individuals with newly diabetes (diagnosis of T2DM [fasting plasma glucose (FPG)≥7.0 mM/L] or impaired fasting glucose [IFG] [FPG 5.6-6.9 mM/L]) were called to participate in the web-based lifestyle intervention via e-mail, and 380 individuals accepted the intervention protocol (intervention group [IG]). The control group (CG, n=97) agreed to participate in post-examination, but received no e-mail on healthy lifestyle to improve T2DM. 448 (CG: 82, IG: 366) of 477 individuals who participated in a health follow-up in 2011, were included in the final analyses.
The web-based lifestyle intervention was developed based on a previous study (16) and guidelines (17, 18). It is detailed in Fig. 1. Participants were encouraged to change unhealthy lifestyle behaviors and eating habits. Each e-mail included information regarding healthy eating habits and lifestyle. After sending each e-mail, the research staff checked within 3 days whether the e-mail had been read. If not read, e-mail material was sent again and short messaging services (SMS) messages were sent to motivate participation.
Measurements
Body height and weight were measured with each subject standing straight wearing light clothing using InBody 720 (Biospace, Seoul, Korea). Body mass index (BMI) was calculated using the body weight (kg)/height (m2). Waist circumference (WC) was measured at the midpoint between the iliac crest and the lower ribs. Blood pressures was measured in duplicate using an electronic sphygmomanometer (FT-700R; Jawon Medical, Seoul, Korea) in a sitting position after a ≥10 min stabilization prior to blood sampling and results were averaged.
Prior to blood sampling, all subjects fasted overnight (more than 10 hr). Blood analysis was performed in a central laboratory (Radiation Health Research Institute). FPG was analyzed by enzymatic methods using commercially available kits and an automatic analyzer (Cobas Integra 800; Roche Diagnostics, Mannheim, Germany). Fasting serum insulin (FSI) was analyzed by radioimmunoassay methods using Irma kit (RALS system, DS8150; ITC Edison, NJ, USA). Hemoglobin A1c (HbA1c) was determined on whole blood samples by VARIANT™ II TURBO HbA1c kit 2.0 and VARIANT™ II TURBO Reagents analyzer (BIO-RAD, CA, USA). The formula for calculating the homeostasis model of insulin resistance (HOMA-IR) was (FSI [µU/mL] ×FPG [mM/L]) ÷ 22.5 (19). Dietary intakes were analyzed using a computerized food frequency questionnaire (FFQ) originally developed by the Korea Centers for Disease Control and Prevention and modified by our institution for industrial workers. The FFQ consisted of 7 food groups including 108 food items. It was designed to collect information regarding the usual food intake over the past one year.
ENPP1 genotyping
We separated the buffy coat from the blood sample of each subject. Genomic DNA was extracted from the above samples using the GENErALL™ Blood SV kit (General Biosystem, Seoul, Korea). Genotyping used to identify the K121Q polymorphism in ENPP1 exon 4 was by polymerase chain reaction-restriction fragment length polymorphism (PCR-RFLP). PCR was carried out in a final volume of 10 µL containing 50 mM KCl, 10 mM Tris (pH 8.3), 1.5 mM MgCl2, 75 ng of each primer, 100 µM deoxy-NTP, and 1 U Taq polymerase. All genotyping was carried out in duplicate for each individual, and the investigator was unaware of the sample origin. In this study sample genotype distribution obeyed the Hardy-Weinberg equilibrium.
Statistical analyses
Power calculations were performed using the G*Power program version 3.0.10 (Franz Faul, Universität Kiel, Germany). A total of 400 subjects were calculated as a sample size for α=0.05 and 95% power among two groups in a two-sided ANCOVA model.
Deviations from Hardy-Weinberg equilibrium at ENPP1 codon 121 were tested by a chi-square goodness of fit test. All the statistical analyses were performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). Data were presented as the mean±standard deviation. Variables with a non-normal distribution were submitted to logarithmic transformation. To compare the differences between CG and IG by ENPP1 polymorphism and differences of changes between KK and KQ+QQ by type of group, independent t-test for continuous variables was applied. In addition, pre-post comparisons were carried out using the paired t-test. ANCOVA was used to compare the clinical and laboratory characteristics of subjects according to genotypes and type of group. Adjustment of changes during intervention comprised the respective pre-values to correct for potential ceiling effects. Multivariate analyses were performed using linear models for gene-by-BMI change interaction in modulating insulin resistance. All two-tailed P values of 0.05 were regard as indicating statistical significance.
RESULTS
Effects of web-based lifestyle intervention on KK genotype
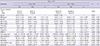
In KK genotype, analytical results in two groups at baseline and 12 months after intervention are shown in Table 1. There were no significant differences between CG and IG except for age, FPG and HbA1c at baseline (Table 1). No differences in anthropometrics, metabolic measurements and nutrient intake at baseline and after intervention were evident for KK CG. However, in the KK IG group, BMI (P=0.022), HbA1c (P<0.001), FSI (P<0.001), HOMA-IR (P<0.001) and intakes of total energy (P=0.019) and protein (P=0.007) were significantly decreased after intervention. Comparison of change of FSI levels between the two groups showed a greater improvement in the KK IG after appropriate adjustment (P=0.033).
Effects of web-based lifestyle intervention on KQ+QQ genotype
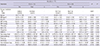
The baseline characteristics and nutrient intakes of the two groups in the KQ+QQ genotype are shown in Table 2. BMI, FSI and intakes of total energy, carbohydrate and total fat were greater in KQ+QQ IG than in KQ+QQ CG at baseline. Intake of carbohydrate was significantly increased in KQ+QQ CG after intervention (P=0.020). In KQ+QQ IG, HbA1c (P<0.001), FSI (P<0.001), HOMA-IR (P<0.001) and intakes of total energy (P=0.002), carbohydrate (P=0.007), protein (P=0.002) and total cholesterol (P=0.044) were significantly decreased after intervention. The web-based lifestyle intervention resulted in significant decrease in HOMA-IR in KQ+QQ IG as compared to KQ+QQ CG after appropriate adjustment (P=0.049).
Magnitude of effect on genotype and web-based lifestyle intervention
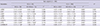
When adjusting for confounders, HbA1c was significantly increased in KQ+QQ CG compared to the KK CG (P=0.038) (Table 3). The reductions in FSI and HOMA-IR were significantly greater in KQ+QQ IG subjects compared to the CG. Similarly, the reductions in KK IG subjects were significantly greater compared to the CG subjects (respectively, FSI: P=0.026, HOMA-IR: P=0.039), and HbA1c reduction were marginally significant (P=0.050).
Relationship between HOMA-IR and BMI changes in IG subjects with T2DM
The relationship between HOMA-IR and BMI was analyzed in IG subjects with T2DM (Fig. 2). When assessed across the two genotypes, the positive correlation was highly significant among 97 KK subjects (adjusted β=0.801; P=0.022) and was not significant among the 18 KQ+QQ subjects (adjusted β=-0.521; P=0.428).
DISCUSSION
In the present study, we demonstrated that web-based lifestyle intervention is effective in improving IR without reference to ENPP1 K121Q polymorphism. Additionally, the K allele has a beneficial effect of weight loss on IR decrease in subjects with T2DM.
IR is one of the main mechanisms implicated in the pathogenesis of both T2DM and metabolic syndrome (20). The HOMA-IR is widely used to estimate IR in large epidemiological studies and in clinical practice (21). Also, the HOMA-IR index correlates fairly well with invasive test of insulin sensitivity and has an acceptable degree of reproducibility (22). Therefore, it has been suggested that HOMA-IR must be assessed as an index of improvement in insulin sensitivity after lifestyle changes (23).
Several studies have reported dichotomous findings concerning the ability of the ENPP1 K121Q polymorphism during lifestyle intervention (13, 14, 24). Recent studies reported that individuals with Q allele benefited more with intervention efficacy (14, 24). However, while the levels of HbA1c and HOMA-IR were significantly reduced in IG, there was no significant difference according to polymorphism in this study. As several previous studies had suggested, different ethnicity may affect environmental and functional genetic factors on other genes (13, 25). Moreover, the Q (risk) allele frequency varies greatly according with the ethnic group (26). Therefore, we suggest that it is important to clarify gene effect in a homogenous racial population.
Energy over-consumption was key to the development of IR and T2DM (27). Macronutrients (calorie nutrients) including carbohydrate, protein and fat have varying effects on blood glucose level (28). Intakes of total energy and fat are closely related with glycemic control (29, 30). Also, effects of dietary change on blood biomarker concentrations differ significantly between individuals. Genetic polymorphisms lead to alteration of the response to dietary components by influencing absorption and metabolism (31). For example, genetic background can interact with habitual dietary fat composition, affecting predisposition to IR syndrome and individual responsiveness to change in dietary fat intake (32). Recently, nutrigenomics raises ethical, legal and social issues particularly with respect to how the public may access nutrigenetic tests and associated nutritional and lifestyle advice (9).
Obesity increases the concentration of insulin in plasma and is the major contributor to IR (33). Increased visceral fat mass may lead to IR in Chinese type 2 diabetic and normorglycemic subjects (34). Moreover, it was recently demonstrated that individuals with elevated body fat percentage have an increased risk of developing cardiometabolic disease despite having a normal BMI (35). In Korean non-obese men, high BMI and waist circumference (abdominal obesity) have been associated with IR (36). Gillies et al. (37) demonstrated that lifestyle modification with weight loss can reduce the incidence of T2DM by up to 58% in populations at risk for T2DM. However, Vogeser et al. (23) showed no correlation between individual change in BMI and change in HOMA-IR during 1 yr of the MOBILIS lifestyle intervention program in obese persons (BMI≥30.0 kg/m2). Maranghi et al. (24) showed that after 6 weeks lifestyle intervention, significant relationship between BMI and HOMA-IR changes according to ENPP1 genotype (β values were 0.34 in 145 KK individuals and 0.85 in 47 KQ+QQ individuals) in Italian men and women. In this study, this correlation was strongly significant among the 97 KK IG with T2DM (adjusted β=0.801). The reasons for this discrepancy may be due to the following differences: 1) intervention type and period (6 weeks, man to man intervention, vs. 10 months, web-based intervention); 2) ethnicity; 3) characteristic of subjects (non-diabetic overweight-obese adults, vs. men with IFG and T2DM); 4) confounding factors (not include dietary change, vs. include dietary change). Intervention type and contact frequency reportedly influence the response to a lifestyle intervention (38, 39). Although data are not shown, BMI were more decreased in the intervention group subjects with T2DM (-0.28 kg/m2) when compared to intervention group subjects with IFG (-0.06 kg/m2) (P=0.039). It is expected that subjects with T2DM would benefit more from HOMA-IR reduction than subjects with IFG.
There were some limitations that need to be addressed. The first is the lack of Q allele subjects. A low proportion of QQ homozygous type is observed in most studies (approximately 2%-3% of the general population) (40). The frequency of the QQ type was very low (1.1%) in our data, so, it prevented appropriately testing of different genetic models (dominant, additive or recessive). Secondly, we did not measure the energy expenditure according to physical activity and exercise, and so were unable to distinguish the additive effects of change in energy expenditure on glycemic control and IR. Nevertheless, this study had the strength in that we tested the ability of ENPP1 to predict intervention efficacy on IR after adjustment for confounding factors such as weight loss and dietary intake. Also, our results provided an interesting concept that is amenable to further study, in terms of a clear effect of genotype.
In conclusion, the ENPP1 K121Q polymorphism is associated with IR during web-based lifestyle intervention, and the K121 allele has a beneficial effect of weight loss on IR. More comprehensive analyses in larger studies are needed to understand the full impact of ENPP1 in Koreans on lifestyle intervention to prevent and delay T2DM.


 XML Download
XML Download