

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
In children with high-risk or recurrent solid tumors, a treatment strategy involving high-dose chemotherapy and autologous stem cell transplantation (HDCT/autoSCT) has shown the potential to improve outcomes (1, 2). Dose escalation using tandem HDCT/autoSCT may further improve outcomes in patients with high-risk or recurrent solid tumors (3-6). Although it is difficult to define the minimum number of stem cells needed for hematologic recovery after SCT, the rate of hematologic recovery is positively associated with CD34+ cell number (7-9) and transplantation of > 5 × 106/kg CD34+ cells improves outcomes (8, 9). When performing tandem HDCT/autoSCT, half of the collected stem cells are infused for bone marrow (BM) rescue during each HDCT/autoSCT session. Therefore, more stem cells are generally needed for successful hematologic recovery when performing tandem HDCT/autoSCT than for single HDCT/autoSCT (10).
The most common method used to mobilize stem cells in children with solid tumors who were scheduled to undergo HDCT/autoSCT is the administration of granulocyte-colony stimulating factor (G-CSF) during the recovery phase of chemotherapy. In a significant proportion of patients (5% to 40%), however, this conventional method induces an insufficient yield of stem cells (11-14). This is of particular concern for patients scheduled to undergo tandem HDCT/autoSCT because this procedure requires larger numbers of stem cells (10).
Various clinical and biological factors may affect stem cell mobilization and collection (15-17), including the time point during recovery after chemotherapy at which PBSC collection begins. However, the optimal time to start PBSC collection has not been established, particularly in children (18). Recently, the number of CD34+ cells in the peripheral blood (PB) is used to decide the timing to start PBSC collection because it can predict PBSC collection yield. However, the number of CD34+ cells in PB may be persistently lower than the threshold level at which PBSC collection begins in poor mobilizers. Therefore, the strategy to start PBSC collection at a certain or higher level of CD34+ cell number in PB might be difficult to apply in poor mobilizers. Therefore, many institutions still consider WBC count in PB as one of valid surrogates. While some studies have suggested initiating PBSC collection when the WBC count in PB exceeds 1,000/µL (19, 20), other studies indicate that waiting until the WBC count is greater than 2,000-10,000/µL may be advantageous (18, 21). For this reason, we performed this study to clarify the optimal timing for PBSC collection in children with high-risk or recurrent solid tumors.
MATERIALS AND METHODS
Patients
First, records of PBSC mobilization and collection between March 1998 and August 2007 for patients with high-risk or recurrent solid tumors who were scheduled to undergo HDCT/autoSCT at Samsung Children's Cancer Center were analyzed to determine the optimal time to initiate PBSC collection. In this early study period, PBSC collection was initiated when the WBC count in PB exceeded 1,000/µL during recovery phase after conventional chemotherapy. Results of this retrospective analysis suggested that initiation of PBSC collection at a higher WBC count in PB might result in a greater CD34+ cell yield. Therefore, during the late study period between September 2007 and December 2012, PBSC collection was initiated only when the WBC count exceeded 4,000/µL during the recovery phase after chemotherapy. Records of patients with hematologic disease, including lymphoma, and of patients treated with G-CSF alone to mobilize stem cells in steady state were excluded from the analysis. In addition, records retrieved during the second collection round in patients who failed to yield a sufficient number of CD34+ cells during the first collection round were also excluded.
Stem cell mobilization and collection
G-CSF was administered starting from the day when absolute neutrophil count (ANC) fell below 500/µL after conventional chemotherapy until the completion of PBSC collection. In the early study period, leukapheresis for PBSC collection was started if the WBC count in PB exceeded 1,000/µL during the recovery phase as described above. In general, leukapheresis was performed using three times the patient's total blood volume through a dual-lumen central catheter unless this presented significant clinical risks for the patient. The aim was to collect at least 2 × 106 CD34+ cells/kg, preferably >5 × 106 CD34+ cells/kg. Irradiated RBCs and platelet concentrates were transfused to maintain a hemoglobin level of 10 g/dL and a platelet count of 50,000/µL during stem cell collection. In the late study period, all collection procedures were identical to those used in the early study period except that PBSC collection was initiated only when the WBC count in PB exceeded 4,000/µL.
Statistical analysis
Differences in the proportions of patients between early and late study periods were analyzed using a chi-square test. Differences in continuous variables between three or more groups were analyzed using the Kruskal-Wallis test. Differences in continuous variables between two groups were analyzed using the Mann-Whitney U test. Multivariate analysis was performed using linear regression analysis to test factors affecting CD34+ cell yield. P values < 0.05 were considered statistically significant.
RESULTS
Patient characteristics
During the early study period, 257 patients underwent PBSC collection. From these patients, we excluded 30 with hematologic disease, 23 in whom stem cell mobilization was induced using G-CSF alone in steady state, and 6 who were treated with GM-CSF for stem cell mobilization. The preliminary analysis of optimal PBSC collection time therefore included 198 patients. During the late study period, 145 patients underwent PBSC collection. From these patients, we excluded 11 with hematologic disease and 9 who were treated with G-CSF alone in steady state. Thus, data of 125 patients were used to confirm results from the early study period.
PBSC collection during the early study period
In the early study period, leukapheresis for PBSC collection was performed for 2-3 days in 75 (37.9%) patients, 4-5 days in 60 (30.3%) patients, and 6-11 days in 63 (31.8%) patients. As expected, PBSC collection was extended when CD34+ cell yield was lower. The WBC count in PB increased as the number of leukapheresis days increased (Fig. 1A). The number of CD34+ cells in PB was positively associated with the WBC count in PB with borderline significance (Fig. 1B). Accordingly, the daily CD34+ cell yield was higher when the WBC count in PB before leukapheresis was higher, specifically at >4,000/µL (Fig. 1C), and the daily CD34+ cell yield increased with the number of leukapheresis days. When assuming PBSC collection had been initiated at peripheral WBC counts exceeding 1,000/µL, 2,000/µL, and 4,000/µL in patients who underwent PBSC collection for 6-11 days, CD34+ cell yield for the first 3 days was highest for initiation at > 4,000/µL peripheral WBC (Fig. 1D). A higher G-CSF dose was not associated with a greater CD34+ cell yield. Collectively, these findings suggest that initiation of PBSC collection at a WBC count of 1,000/µL may be too early for optimal yield and that waiting until WBC count exceeds 4,000/µL may be advantageous.
PBSC collection during the late study period
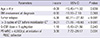
Therefore, in the late study period, we initiated PBSC collection when the WBC count in PB exceeded 4,000/µL. Data of patients treated in this period were analyzed to test preliminary conclusions derived from the early study period. Patients in the late study period were older than those in the early study period (Table 1). The most frequent diagnosis was neuroblastoma; however, the proportion of brain tumors was higher and a lower dose of G-CSF was used in the late study period. The two study groups did not differ in the proportion of patients with relapsed tumor, the proportion with BM involvement at diagnosis, the interval between initial diagnosis and PBSC collection, and the processed blood volume during leukapheresis. As results, there were fewer leukapheresis events in the late study period than in the early study period (median 3 [range 2-10] vs median 4 [range 2-11], P < 0.001). Daily yields of total nucleated cells and CD34+ cells were higher in the late study period, and the total yields of total nucleated cells and CD34+ cells were higher despite the shorter collection period in the late study period. Similarly, the proportions of patients from whom > 5 × 106 CD34+ cells/kg and > 10 × 106 CD34+ cells/kg were collected were higher in the late study period than in the early study period. When the analysis was performed according to the number of PB WBC at initiation of PBSC collection during both early and late study periods, results were similar (Table 2). When hematologic recovery after mobilization chemotherapy was delayed, in other words, when the interval between initiation of mobilization chemotherapy and initiation of PBSC collection increased, CD34+ cell yield decreased (P < 0.001).
Multivariate analysis for factors affecting CD34+ cell yield was performed using data from all patients during both early and late study periods (Table 3). In the multivariate analysis, tumor relapse and longer chemotherapy before mobilization chemotherapy (> 3 cycles) independently predicted poor CD34+ cell yield. Initiation of PSBC collection after the WBC count in PB exceeded 4,000/µL was independently associated with a greater CD34+ cell yield. Age, BM involvement of tumor at diagnosis, and G-CSF dose were not independently associated with CD34+ cell yield.
Hematologic recovery after HDCT/autoSCT
In the early study period, 176 patients underwent the first HDCT/autoSCT, and 125 of these underwent the second HDCT/autoSCT. In the late study period, 108 patients underwent the first HDCT/autoSCT, and 96 of these underwent the second HDCT/autoSCT. The numbers of CD34+ cells infused in the first and second HDCT/autoSCT were higher in the late study period than those in the early study period. Accordingly, neutrophil recovery in both the first and second HDCT/autoSCT and platelet recovery in the first HDCT/autoSCT were faster in the late study period than in the early study period (Table 1).
DISCUSSION
Although the number of CD34+ cells in PB can predict PBSC collection yield, many institutions still consider WBC count in PB as one of valid surrogates to decide the timing to start PBSC collection because the number of CD34+ cells in PB may be persistently lower than the threshold at which PBSC collection begins in poor mobilizers, and therefore, the strategy using the number of CD34+ cells in PB as valid surrogate to decide the timing to start PBSC collection might be difficult to apply in poor mobilizers. However, the optimal WBC count in PB to start PBSC collection has not been systematically tested, particularly in children with high-risk solid tumors (18). In this context, we retrospectively reviewed data of PBSC collections conducted during two study periods that differed in the threshold WBC count in PB at which leukapheresis was initiated. Our findings indicated that deferring PBSC collection until the WBC count in PB exceeds 4,000/µL may be advantageous for CD34+ cell yields. Results in the late study period validated our conclusion from the early study period. Collection of a higher number of CD34+ cells was associated with a faster hematologic recovery after transplant in the late study period. Multivariate analysis showed that initiation of PBSC collection after the WBC count in PB exceeded 4,000/µL independently predicted a higher CD34+ cell yield.
The use of tandem HDCT/autoSCT to treat high-risk or recurrent solid tumors in children is currently increasing (3-6). For this procedure, the number of CD34+ cells collected is of particular concern because the number of cells transplanted during each session may be lower than the number transplanted when only a single HDCT/autoSCT is performed. In our experience, platelet and RBC recoveries are significantly delayed in the second HDCT/autoSCT compared with the first HDCT/autoSCT, but this delay may be overcome if a sufficient number of CD34+ cells (> 5 × 106 cells/kg) can be transplanted in each session of tandem HDCT/autoSCT (10). The present study showed that the proportions of patients from whom > 5 × 106 CD34+ cells/kg and >10 × 106 CD34+ cells/kg were collected were significantly higher when PBSC collection was delayed until WBC counts exceeded 4,000/µL.
The patient groups analyzed in the two study periods presented some clinical differences that may potentially have influenced CD34+ cell yields. However, initiation of PBSC collection at a higher WBC count independently predicted higher CD34+ cell yield in the multivariate analysis of data from all patients included in both early and late study periods. In addition, tumor relapse and extended chemotherapy before PBSC collection were independently associated with a lower CD34+ cell yield. These findings suggest that early collection of stem cells may be preferred if the possibility of tumor cells in circulation can be ruled out. It is also interesting that bone marrow involvement of the tumor at diagnosis and G-CSF dose were not independently associated with CD34+ cell yield in the present study.
While our analysis shows that a higher initial WBC count promotes a higher stem cell yield, collection of CD34+ cells in therapeutic numbers presents a challenge in some patients. For patients recognized as "poor mobilizers", the macrocyclic compound plerixafor may boost CD34+ cell yield. In adults, more CD34+ cells could be collected with G-CSF + plerixafor than with G-CSF alone (22-26); however, the efficacy and toxicity of plerixafor have not been established in children with solid tumors. Furthermore, most studies describe the use of plerixafor in the steady state without mobilization chemotherapy. Therefore, if plerixafor is to be used during hematologic recovery following mobilization chemotherapy, it may be necessary to determine not only the optimal time to initiate PBSC collection, but also the time to start plerixafor treatment.
In conclusion, delay in the initiation of PBSC collection until the WBC count in PB exceeds 4,000/µL is associated with a higher CD34+ cell yield, and consequently a faster hematologic recovery after HDCT/autoSCT, particularly in tandem HDCT/autoSCT. Further studies to confirm our findings may be justified.



 XML Download
XML Download