

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The diagnosis of idiopathic interstitial pneumonia (IIP) requires exclusion of other known causes of interstitial pneumonia, including drugs or other environmental exposures and connective tissue disease (CTD) (1). All types of IIP, except respiratory bronchiolitis associated with interstitial lung disease (RB-ILD), can occur in CTDs and the prognosis of CTD-related interstitial pneumonia (CTD-IP) is reported to be better than that of IIP (2). Therefore, most clinicians routinely do serologic testing for CTD such as antinuclear antibody (ANA) and rheumatoid factor (RF), in addition to detailed history taking and physical examination at the time of diagnosis (3). Recently, American Thoracic Society (ATS)/European Respiratory Society (ERS)/Japanese Respiratory Society (JRS)/Latin American Thoracic Society (LATS) guidelines for idiopathic pulmonary fibrosis (IPF) have recommended the testing of autoantibodies as an initial diagnostic procedure. However, there are no reliable data on the role of screening autoantibodies in patients with suspected IIP. Furthermore, some patients with CTD-IP may present as IIP without any clinical signs of CTD at the time of initial diagnosis and the manifestations of CTD will be apparent during a later follow-up (4). However there are no data on the incidence of new CTD arising in IIP cases, except in the case of nonspecific interstitial pneumonia (NSIP), and it is not yet clear whether the presence of autoantibodies anticipates the evolution of overt CTD or predicts future prognosis.
The aim of this study was to investigate whether the presence of autoantibodies has: 1) any prognostic value for mortality; and 2) predictive value for the development of overt CTD in patients with IIP.
MATERIALS AND METHODS
Subjects
The present retrospective study included 688 patients (526 with IPF, 85 with NSIP, and 77 with cryptogenic organizing pneumonia [COP]) diagnosed from January 1995 to December 2009 at Asan Medical Center, Seoul, Korea according to the ATS/ESR classification (1). Usual interstitial pneumonia (UIP) patterns were confirmed by surgical lung biopsy (294 patients, 55.9%) and/or high-resolution computed tomography (HRCT). Both NSIP and COP were diagnosed by surgical lung biopsy. Patients with a history of drug toxicity, or exposure to environmental agents known to cause interstitial lung disease, or overt CTDs were excluded. Diagnosis of rheumatoid arthritis (RA) (5), and systemic lupus erythematosus (SLE) (6) were based on the ACR criteria. Dermatomyositis (DM) and polymyositis (PM) were diagnosed according to the Bohan-Peter criteria (7). The LeRoy and Medsger criteria, the American-European criteria and the Alarcon-Segovia and Cardiel criteria were used for the diagnosis of systemic sclerosis, Sjogren's syndrome, and mixed CTD respectively (8-10). Undifferentiated connective tissue disease (UCTD) was diagnosed, if the patients had suggestive symptoms or signs with positive autoantibody result but did not fulfill the diagnostic criteria for a specific rheumatic disease (11). Anti-neutrophil cytoplasmic antibody (ANCA)-associated vasculitides was diagnosed based on the ACR classification and the Chapel Hill consensus (12-14). Although this was a retrospective study, a thorough systematic history (see Table E1, online supplemental data), physical examination, and serological testing for CTD were performed at the time of initial diagnosis in all patients suspected of CTD and also intermittently during follow-up.
Methods
The biopsy slides were reviewed independently by at least two pathologists who were blind to the clinical findings. The HRCT images were reviewed by radiologists also in a blind manner. All diagnoses were made using a multidisciplinary approach that included experienced clinicians, radiologists, and pathologists. The majority of the patients with IIP in our current study cohort have been analyzed in our previous studies (2, 15-17). All of the current data were obtained from medical records, and the survival status was obtained from hospital medical records, the records of National Health Insurance of Korea, and/or through telephone interviews. Most of the clinical parameters were obtained within one month of surgical lung biopsy or HRCT.
Antinuclear antibody
ANA was tested in the serum using a commercially available pre-standardized kit (ANA/HEp-2 Test System; Zeus Scientific, Inc., Raritan, NJ, USA). If the serum tested positive in the initial 1:40 dilution, it was serially titrated to 1:1,280. Autoantibodies against extractable nuclear antigens (ENAs) were tested using an ENA Combi ELISA kit (BL Diagnostika, Mainz, Germany). A signal-to-cut-off ratio greater than 1.0 was considered positive.
Rheumatoid factor
RF was measured using a commercially available kit (RapiTex RF; Dade Behring Inc., Deerfield, IL, USA) that uses slide latex agglutination for qualitative measurements. A positive agglutination reaction indicated the presence of at least 20 IU/mL in the serum.
Anti-citrullinated protein and anti-neutrophil cytoplasmic antibody
Anti-citrullinated protein (anti-CCP) was measured using a commercially available kit (EliA CCP; Phadia inc., Uppsala, Sweden) that uses an enzyme immunoassay. A positive reaction was indicated by at least 10 U/mL CCP in serum. ANCA was measured using a commercially available kit (EliA Well; Phadia inc., Uppsala, Sweden). A positive reaction for myeloperoxidase (MPO)-ANCA was considered to be at least 3.5 IU/mL, whereas a minimum reading of 2.0 IU/mL was required for proteinase-3 (PR3)-ANCA positivity.
Statistical analysis
All values are described as the mean ± standard deviation. A chi-square test or Fisher's exact test was used for categorical data, and an unpaired Student's t-test or Mann-Whitney test was used for continuous data. P values less than 0.05 were considered statistically significant (two-tailed). Statistical analyses were done using SPSS version 18.0 (SPSS, Chicago, IL, USA).
RESULTS
Frequency of autoantibodies detected in patients with IIP
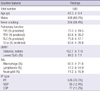
The mean age was 61 yr and 68.0% were male (Table 1). The median follow-up period was 33.6 months (IQR, 16.3-62.1 months).
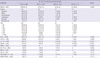
ANA and RF were evaluated in more than 90% of the subject patients and most of the specific antibodies were also tested in the majority of the patients, with exception of anti-CCP antibody which was measured in just 192 subjects (27.9%). Approximately one-third of the patients (223, 34.5%) were positive for ANA and 13.2% had positive RF results. However, the prevalence of most of the specific autoantibodies was low (between 0.7% and 6.8%). ANA positivity was more frequent in the NSIP group compared with the other groups (Table 2).
In patients with IPF, a speckled pattern was the most common. The ANA titer was available in 547 patients, including ANA-negative (< 1:40) patients. The majority of the patients had a low ANA titer (less than 1:80), and only 30% had a titer higher than 1:320 (Table 2).
Comparisons of the clinical features of IIP patients according to the presence of autoantibodies
Among the patients who were positive for ANA, females and never smokers were predominant (Table E2, online supplemental data). Patients with positive ANA titers had a lower lung function and a tendency towards a higher lymphocyte percentage in bronchoalveolar lavage (BAL) fluid than ANA-negative cases. There were no significant differences between the RF (+) and RF (-) groups other than a higher percentage of neutrophils in the BAL fluid of RF (+) patients.
Because the prognostic value of autoantibodies is more important in IPF than in any other types of IIP, we only analyzed and compared the outcome for IPF. The median survival outcome was not significantly different between the ANA-positive and ANA-negative groups (40.6 vs 46.2 months) (Table E2, online supplemental data). The one- and three-year survival rates for ANA-positive patients (83.9% and 67.0%, respectively) were also not found to be significantly different from those of ANA-negative patients (1-yr, 85.4%; 3-yr, 65.2%; P = 0.155). The result was the same when only the patients with higher titers of ANA were categorized as the positive group. Similarly, in all patients including those with NSIP and COP, no significant difference in survival was found between the ANA-positive and -negative patients (data not shown).
Development of overt CTD during follow-up
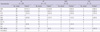
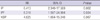
Of the 688 patients in our current study cohort with IIP, 26 cases (3.8%) developed overt CTD: 2.5% in IPF, 6.5% in COP, and 9.4% in NSIP (Table 3). Rheumatologic consultation was done for all patients at the time of CTD diagnosis but not initially, because they did not have any symptoms suggestive of CTDs. RA was the most common CTD (all in the IPF group), followed by Sjogren's syndrome and PM/DM (Table E3, online supplemental data). Two patients who were positive MPO-ANCA (one with IPF and one with COP) developed vasculitis (microscopic polyangiitis). CTD development was higher in the ANA-positive group (8.5% in IIP, 6.4% in IPF) than the ANA-negative group (1.7% of IIP, 0.9% of IPF; P = 0.001). Most of the patients (73.1%) who developed CTD had positive ANA titers at the time of the initial diagnosis of IIP (Table 4), which was significantly higher than the prevalence in all subjects (34.5%)(Table 2). Moreover, the frequency of CTD development correlated with an increasing ANA titer (data not shown): the relative risk for a titer higher than 1:320 was 6.431 (95% CI, 2.340-17.569; P = 0.002) (Table 5).
Regarding specific autoantibodies, the frequency of positivity of anti-SSA (20.8%), anti-CCP (33.3%), and MPO-ANCA (13.0%) was significantly higher in the patients who developed CTD. In addition, the frequency of CTD development was higher in the patients who were positive for specific autoantibodies (16.3 vs 2.1%; P < 0.001), especially in cases positive for anti-CCP and anti-SSA (anti-CCP, 53.8%; anti-SSA, 16.1%), when compared with the no CTD group (7.8%, and 3.6%, respectively; Table E4, online supplemental data).
DISCUSSION
The results of our current study show that in IPF, the presence of autoantibodies has no significant predictive value for survival. However, autoantibodies were found to be predictive for the future development of CTD, although the incidence of newly developed CTD was low in our patient series. The majority of our patients who developed CTD had a positive ANA titer, and the frequency of new CTD was significantly higher among patients who were positive for ANA (> 1:320), anti-CCP, and anti-SSA.
Although it is well known that CTD-IP has a better prognosis than IPF and that some patients with IIP develop CTD during follow-up, the true relationship between autoantibodies and an IIP prognosis has not been clear to date. This relationship is more critical in patients with a UIP pattern because of the poor prognosis associated with IPF and the much better prognosis for cases of CTD-related UIP. Recently, we reported that the prognosis was similar in IPF patients with and without autoantibodies, although the pathological features of patients with IPF and positive autoantibodies were closer to those of CTD-UIP cases than to IPF cases without autoantibodies (17). Because of the small number of subjects in that study (n = 100), we recommended further investigation with a larger cohort. In our present study, which analyzes a much larger number of patients, no relationship between survival and autoantibodies could be confirmed. Although the result was negative, this is the first reliable data obtained from large number of the patients with a relatively long-term follow-up period.
Although conducted before the ATS/ERS consensus classification was developed, many previous studies have reported a high prevalence of ANA and RF positivity (6, 18-22), and which was also recently confirmed by Fischer et al. (23) for surgical lung biopsy proven IPF. The prevalence was higher in idiopathic NSIP (24) and similar results were obtained in our present study. ANA is also present in healthy individuals (25-27); 1:40 in 25%-30%, 1:80 in 10%-15%, and 1:160 or greater in 5% (27). In our current study, the prevalence of a low titer of ANA was similar but the prevalence of a high titer of ANA seemed to be higher than previously reported value (Table 2). Moreover, whereas Fischer et al. (23) have reported that a nucleolar pattern is predominant (26%) in IIP with a frequent development of scleroderma. Mitoo et al. (24) reported that a speckled pattern was predominant in these cases without any development of scleroderma, similar to the findings in our present study.
The incidence of CTD in our patients series was found to be low, with only 2.5% in IPF patients (3.8% in IIP), compared with the 19.1% reported by Homma et al. (4) and the 17.5% reported by Mittoo et al. (24). However, the subject numbers in those two studies were relatively small (n = 13) (4), or (n = 97) (24) and they included other types of interstitial lung disesase with significant referral bias by study design. Despite the low incidence of CTD, our study results show that CTD-development is closely associated with ANA; not only was there a higher incidence of CTD in the ANA-positive group than in the ANA-negative group (8.5% vs 1.7%, respectively; P = 0.001), but there was also a higher initial positivity for ANA in the CTD-development group compared with the non-CTD group. Our results also provide supporting evidence for accepting an ANA titer > 1:320 as a provisional criterion for lung dominant CTD, as proposed previously by Fischer et al. (28).
Mittoo et al. (24) have reported that inflammatory myositis is the most common new CTD. In our present study however, this condition developed in only three patients; one with NSIP and two with COP, and no patients with in IPF. Because of the unavailability of anti-synthetase antibody test for our present analyses, we cannot exclude the possibility of misdiagnosis. However, we paid particular attention to the clinical features of that disease in concert with our rheumatology colleagues and considering rapid (less than one year) development of inflammatory myositis reported by Mittoo et al. (24) the chance of misdiagnosis is likely to be low. In our present study, the most common type of subsequent CTD was found to be RA in IPF, consistent with the observation that the UIP pattern is the most frequent pathological pattern in RA-IP patients. The anti-CCP antibody test was introduced late into our study and was therefore performed in only one-third of the patients. However, about half of the patients who developed RA were positive for the anti-CCP antibody at the initial evaluation without showing any clinical features of RA. Hence, our results also indicate that anti-CCP positivity is a predictor for RA (29-31).
Classically, specific autoantibodies are considered to be highly specific for the diagnosis of certain rheumatologic diseases (32, 33). A few of our patients were positive for specific autoantibodies but without any evidence of CTD or vasculitis (Table 4). Four of these cases developed CTD that was specific for the corresponding autoantibody, such as anti-RNP for MCTD or anti-SSA for Sjogren's syndrome, and two patients with positive MPOANCA developed vasculitis (microscopic polyangiitis). In contrast to ANA (24-26), only a few previous studies have reported the prevalence of specific autoantibodies in non-CTD individuals; anti-Ro, 2.7%-10.2% (33, 34), anti-La, 0.9% (34), anti-Scl70, 0%-3% (35, 36), anti-Sm, 0%-0.5% (34, 35), which are similar to our results.
Another value of autoantibody testing is in providing clue to a possible unrecognized CTD. Our study was not designed to evaluate this possibility. However, Mittoo et al. (24) have reported that 71% of the patients they analyzed with a newly diagnosed CTD had a positive ANA titer, in contrast to a 45% positivity level in non-CTD patients. Related to this, Castelino et al. (37) have reported that among 15 patients referred to as IPF, seven were diagnosed as CTD and all were ANA-positive. Despite being limited by the small numbers of patients examined, these earlier reports showed that a significant number of patients with IIP may have an unrecognized CTD and that a positive ANA result may have utility as a warning signal for CTD.
A positive RF result has been previously reported in 4% of young healthy individuals (38) and in 3%-25% of elderly subjects without rheumatologic diseases (39, 40). Considering the mean age of our patients, the prevalence of RF positivity in our patients is similar to that of elderly people. Although we observed that CTD development was higher in patients who were positive RF, most of the patients were in the NSIP group.
Our present study has several limitations. Because this is a retrospective study, and despite of all the efforts to exclude CTD at the initial diagnosis, there is still a possibility that CTD was missed in some cases, especially inflammatory myositis and UCTD. Although we used a checking assessment protocol for CTD, there remains the possibility that minor symptoms and/or signs had been missed by either the patients themselves or their physicians. In addition, we could not check the presence of myositis associated specific antibodies. However, a thorough systematic review of patient symptoms, physical examination, and serological testing for CTD with frequent rheumatologic consultation were performed in the majority of the patients at the time of initial diagnosis and again during follow-up. Therefore the possibility that we failed to exclude CTD patients is less likely. Another possibility is that the development of CTD was masked by immunosuppressive therapies administered after the initial diagnosis. However, most of the patients with IPF in our present study were not treated, and if treated, the duration was only briefly. Therefore this possibility that CTD development was masked by immunosuppressive therapies is again less likely. Another noteworthy possible limitation is the relatively short follow-up duration (median, 33.6 months). However, considering the short survival period associated with IPF and the high proportion of IPF case in our cohort, our follow-up period may be reasonable for the purpose of these analyses. Nonetheless, it may be too short for the development of CTD, as it usually takes more than 10 yr in patients with autoantibodies to develop overt CTD. This may be one possible explanation for the low incidence of CTD development in patients with autoantibodies in our study. Despite these limitations, our study provides a robust analyseis of the incidence of newly arising CTD in patients with IIP, particularly IPF, and also the clinical significance of autoantibodies.
In conclusion, our current findings shows that the presence of autoantibodies, especially ANA with a titer > 1:320, and anti-CCP and anti-Ro antibody positivity is clinically useful for predicting the future development of CTD in patients with IIP, although theses factors have no significant predictive value for mortality.

 XML Download
XML Download