

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The introduction of highly active antiretroviral therapy (HAART) has led to dramatic improvement in survival for persons living with human immunodeficiency virus (HIV), turning a fatal disease into a manageable chronic condition (1-3). In HIV infected patients without other risk factors on a successful HAART, the probability of survival is approaching closer to that in the general population of a similar age (4-9). Along with increased survival, the causes of death among HIV-infected patients also have gradually changed. As a result of the dramatic reduction in mortality due to acquired immunodeficiency syndrome (AIDS) defining illness, the proportion of non-AIDS-related death has increased in HAART era (10-12).
In Korea, a total of 7,656 individuals were diagnosed with HIV infection between 1985 and 2010, and 1,364 (17.7%) of whom died (13). Since the first introduction of zidovudine in 1991, antriretroviral agents were sequentially introduced in Korea; other nucleotide reverse transcriptase inhibitors (didanosine in 1994, lamivudine in 1997, stavudine in 1999, and abacavir in 2002), followed by protease inhibitors (indinavir in 1997, nelfinavir in 1998, lopinavir/ritonavir in 2001, atazanavir in 2005 and darunavir in 2010), non-nucleotide reverse transcriptase inhibitors (efavirenz in 1999, and nevirapine in 2000), and an integrase inhibitor (raltegravir in 2010). The survival following HIV diagnosis continue to be improved over time in HAART period in Korea (14). However, proportion of deaths within 6 months of HIV diagnosis increased from 13.3% in pre-HAART era (1985-1996) to 59.2% in HAART era (1997-2007), suggesting that late presentation was an important risk factor for early death among HIV-infected individuals in Korea (14). Moreover, another recent study showed that 41% of newly diagnosed HIV infected individuals in Korea presented with advanced HIV disease, and proportion of late presentation increased after abolition of a government policy of mass mandatory screening, from 31.3% in 1987-1998 to 43% in 1999-2008 (15). Although an increase in survival has been documented, there are no published data comparing specific causes of death between pre-HAART era and HAART era in Korea. The objective of this study was to assess the trends in mortality rate and cause of death over time among HIV infected patients in Korea between pre-HAART era and HAART era.
MATERIALS AND METHODS
Study population and design
A retrospective hospital-based cohort study was conducted to assess mortality and causes of death among HIV-infected patients. Pusan National University Hospital is a 1,220 bed, university-affiliated teaching hospital and provides HIV care for HIV infected patients in southeastern area of Korea, in close collaboration with local Public Health Centers (PHCs) in this area. The study included patients aged 18 yr and older who attended the study hospital for the first time for HIV care between 1990 and 2011. Patients who had received medical care for HIV and/or had taken antiretroviral therapy in other hospitals before they referred to the study hospital were excluded. The survival of patients who did not receive regular follow-up at study hospital was verified by local PHCs in their local district.
Three study periods were defined; pre-HAART period (1990-1997), early-HAART period (1998-2001), and late-HAART period (2002-2011). The patients were retrospectively classified according to the treatment period in which they were recruited, and their characteristics were analyzed separately. The initiation of HAART and prophylaxis for opportunistic infections (OIs) were based on international guidelines (16-18).
Definitions
Cause of death was defined as the main conditions that initiated the sequence of events resulting in death. Cause of death was determined by the infectious disease specialist who had taken care of the patient if the patient died in the study hospital. If the patient died in other hospitals, the first author determined the cause of death by reviewing the medical records. If the hospital records were unavailable or the patient did not die in a hospital, the cause of death was determined from death certificates. Cause of death was categorized as an AIDS-death if the stated cause was an AIDS-defining OI or malignancy. AIDS-defining illness and clinical categories were defined by the 1993 Centers for Disease Control and Prevention (CDC) classification criteria (19). Cause of death was classified as a non-AIDS death for patients who died of other conditions, which was further categorized into bacterial infection/sepsis, non-AIDS-related malignancy, cardiovascular disease, liver disease, pulmonary disease, gastrointestinal disease, renal disease, hematological disease, and accidental cause, including accident, injury and suicide. We considered the cause of death to be indeterminate if the stated cause of death was nonspecific, such as cardiopulmonary arrest, AIDS or HIV infection without further specification, pneumonia of unknown etiology, and encephalitis of unknown origin. Death was classified as unknown cause if there were no available death certificates or no data in local PHCs. Tuberculosis was classified as definite, probable, or possible: definite if culture for Mycobacterium tuberculosis was positive; probable if clinical symptoms and signs consistent with tuberculosis were present and stain was positive for acid-fast bacilli or if there were histological findings consistent with tuberculosis; possible if clinical and radiological signs consistent with tuberculosis were present and there was improvement with standard antituberculous therapy (20). Other opportunistic diseases including Pneumocystis pneumonia (PCP) were diagnosed according to the criteria suggested by the CDC (19). Hepatitis B virus (HBV) infection was defined as positive HBV surface antigen in the serum. Hepatitis C virus (HCV) infection was defined as the presence of HCV antibody with positive RNA in serum.
Statistical anlaysis
Categorical variables were compared using Pearson's chi-square test or Fisher's exact test, whereas non-categorical variables were tested with the Mann-Whitney U-test or the Kruskall-Wallis test. The mortality rate for each group was calculated as the number of deaths per 100 person-years (PY) of observation. Survival duration was calculated from the date of first visit to the study hospital for HIV care to the date of death, or December 31th 2011. The relationship between the treatment period in which they were recruited and survival rate was assessed using the Kaplan-Meier method compared by log-rank test and generalized Wilcoxon test stratified by the treatment period in which they were recruited. All tests were considered statistically significant at P < 0.05. The statistical analyses were conducted using PASW Statistics 18 (SPSS Inc., Chicago, IL, USA) and STATA 11.1 (StataCorp LP., College Station, TX, USA).
RESULTS
Subjects
Between 1990 and 2011, a total of 841 patients attended the study hospital. Of these, 94 patients who had received medical care for HIV and/or had taken antiretroviral therapy in other hospitals before visiting study hospital were excluded, leaving 747 patients for analyses. These 747 patients were grouped according to the treatment period in which they were recruited; 103 in pre-HAART period, 105 in early-HAART period, and 539 in late-HAART period. The baseline characteristics of the 747 patients are shown in Table 1.
Mortality
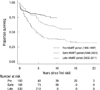
Of the 747 patients, a total of 222 patients (29.7%) died during the study period; 67% (69/103), 43.8% (46/105) and 19.9% (107/539) of the individuals presented in pre-HAART, early-HAART, and late-HAART period, respectively. Of the 222 patients who died, 154 (69.4%) died in hospital (120 in the study hospital and 34 in other hospitals) and 52 (23.4%) at home. Mortality rates per 100 person-year (PY) declined from 8.7 (95% CI, 6.86-10.99) in pre-HAART period to 5.4 (95% CI, 4.07-7.25) in early-HAART period, which further declined to 4.9 (95% CI, 4.05-5.91) in late-HAART period (generalized Wilcoxon test: chi-square test value of 28.8 on 2 degree of freedom, unadjusted P < 0.001). There was a higher risk of death at early time points in patients presenting in late-HAART period compared with those who presented in both pre-HAART and early-HAART period (Fig. 1). Changes in demographic characteristics of those dying over three periods were broadly in line with changes in the baseline subjects (Table 2). In addition, the proportion of deaths within 3 months of presentation significantly increased over the three periods from 15.9% in pre-HAART period to 55.1% in late-HAART period (P < 0.001).
Causes of death
Of the 222 patients who died during study period, 59% was attributable to AIDS-related conditions and 29.3% to non-AIDS related conditions (Table 3). Although the proportion of non-AIDS-related deaths increased from 23.2% in patients presented in pre-HAART period to 41.3% in patients presented in early-HAART period, a trend toward a further rise in non-AIDS-related death rate did not occur over time in late-HAART period (28%) (P=0.117). Overall, PCP was the most common cause of AIDS-related death (20.3% of all deaths), and invasive bacterial infection (6.8% of all deaths) was the most frequent non-AIDS related conditions as cause of death. The proportion of patients who died as a result of PCP increased over time from 8.7% in pre-HAART period to 10.9% in early-HAART period, further a profound rise to 31.8% in late-HAART period (P<0.001). In contrast, the proportion of deaths due to tuberculosis gradually decreased over time from 20.3% in pre-HAART period to 17.4% in early-HAART period, further dropped to 13.1% in late-HAART period (P=0.410).
DISCUSSION
In this study, we had a longitudinal follow-up over 20 yr to monitor the changes in survival and cause of death among the HIV-infected patients in Korea. In order to make more accurate estimates of actual survival, we traced all the patients lost to follow-up after initial linkage to HIV care to determine definitive outcomes of these lost patients because mortality rates may be underestimated if patients are not actively traced (21). This study showed that the survival of patients presenting to the hospital for HIV care in HAART era significantly improved compared with those who presented in pre-HAART era. These findings are generally consistent with findings of other studies conducted in developed countries (1-3), and in Korea (14). In our study, even during HAART period, survival of the patients presenting in late-HAART period improved than that of the patients presenting in early-HAART period. However, as shown in Fig. 1, in spite of survival improvement in HAART era, the early mortality was still substantial in late-HAART period. This is presumably due to high proportion of patients presenting late into care. More than 50% of patients presenting in late-HAART period, furthermore, more than 70% of patients who died among them had a CD4 cell counts ≤200 cells/µL at first presentation for HIV care. The duration from HIV diagnosis to presentation for care decreased significantly over time, whereas the proportion of patients presenting with advanced HIV disease increased over time, indicating that the actual diagnosis of HIV infection occurs almost as late as their initial presentation for care in late-HAART period. These findings are also consistent with the findings of the previous study conducted in Korea, in which 59.2% of all deaths occurred within 6 months of HIV diagnosis in HAART period (1997-2007) (14).
The pattern of the cause of death was broadly in line with these findings. We could not observe the shift of cause of death toward non-AIDS-related death in HAART era, which had been demonstrated in other studies conducted in Western countries (1, 10-12, 22-26). The proportions of AIDS-related death remained higher than non-AIDS-related death in all three periods. Although the proportion of non-AIDS-related death in HAART period increased compared to pre-HAART period, there were no significant changes across the three study periods, rather it decreased in the late-HAART period compared to the early HAART period. For each cause of death in non-AIDS-related death, there were no significant changes in frequency across the three periods, including those that require a longer time to lead to death, such as cardiovascular disease, non-AIDS malignancy, liver disease.
In our study, PCP and tuberculosis were the most common causes of death. However, there was a trend toward increasing number of PCP and decreasing frequency of tuberculosis as cause of death over time. These findings seem to be the result of the increase of the proportion of late presenter to care in late-HAART period. After widespread use of prophylaxis and HAART, the majority of cases of PCP occur among patients who are unaware of their HIV infection or are not receiving ongoing HIV care (27-30). In this study, 82,4% of deaths due to PCP among patients enrolled in late-HAART period occurred at the time of their first presentation for HIV care. Their baseline median CD4 cell count at the initial presentation was as low as 21 cells/µL, and only 32.4% of them received HAART.
This study has several limitations. First, our study was conducted at a single center in the southeastern area of Korea, and therefore our findings may not be generalized to other regions of the country. Second, because our study was based on the population presented to the hospital for HIV care, AIDS-related death might be overestimated. Third, this study allowed us to monitor long-term trends of mortality and cause of death, however, we were not able to perform a more detailed analysis of the causal role of the specific risk factors related to death, such as underlying conditions, lost to follow-up rate, the effectiveness of prophylaxis and HAART, or the effect of the immune reconstitutional inflammatory syndrome.
In summary, we observed a significant improvement of survival of the HIV-infected patients in HAART era. Despite of this improvement, there is still a high risk of death at early time points in patients presenting in late-HAART period, mainly due to late HIV diagnosis and late presentation to care. The spectrum and changing patterns of the cause of death is also largely reflective of these results. Since AIDS-related death still remains the leading cause of death, further research is needed to identify the specific risk factors related to death in HAART era.



 XML Download
XML Download