

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Recently, suicide is a major mental health issue in Korea (1). Suicide is the fourth highest cause of death in Korea with an average of 42 incidents a day (2). The identification of the risk factors of suicide has therefore become a crucial target in health policy.
A number of studies have examined suicide risk factors, prevention and the ways of reducing suicide-related behaviors. Previous studies have shown that suicide is the result of a multifaceted range of social, psychiatric and biological factors, and one or more of these variables may affect suicidal behaviors by complex mechanisms (3-5). Although there are many studies of suicidality and suicide risk factors in people with various mental disorders (6, 7), the findings of these researches may not necessarily generalize to the general population.
The problem of suicide is no longer limited to some psychiatric patients, and consequently the assessment of suicidality and preparing for its appropriate management in the community has important clinical implications (8). For the sake of the mental health of the community, it is therefore necessary to conduct a study of risk factors for suicide idea in the general population sample at large rather than just on those psychiatric patients receiving hospital inpatient or outpatient services. This will enable us to plan suicide prevention strategies not only for psychiatric patients, but also for people in the general community, who do not visit mental health services.
Thus, the main purpose of the present study was to assess suicidal ideation and related factors in a community sample, which was representative of the general population in an urban area of Korea.
MATERIALS AND METHODS
Subjects
The current study was conducted as a part of the community mental health survey in Incheon, a metropolitan city in Korea. The subjects (sample size: 1,116 participants) were sampled with randomization and recruited by a research agency from all eight administrative districts of the city. The number of subjects recruited from each district was proportional to the relative population size of the district. For each district, equal numbers of males and females and equal numbers of subjects in four different age-groups (the 20s, 30s, 40s, and 50s) were sampled. Fifteen trained surveyors made contact with the subjects. They were educated 2-hr about content of self-report questionnaires used in this study and basic psychiatric concepts including depression and suicide before the interview. The final enrollment comprised a representative population sample of 1,000 people aged over 20 yr (Table 1; 500 males and 500 females; mean age of total sample 39.6 ± 11.6 yr ranging 20-59 yr). All participants completed self-report questionnaires including sociodemographic information, the Center for Epidemiologic Study Depression Scale (CES-D), the Beck Scale for Suicide Ideation (BSI), the Spielberger State-Trait Anger Expression Inventory (STAXI), the Barratt Impulsiveness Scale (BIS) and questions on sleep duration on weekdays.
Measures
Depressive symptoms were assessed with the Korean version of the CES-D (9), which was originally developed for use as a screening instrument to identify people at risk for clinical depression (10). The scale includes 20 items, which measure the presence and severity of depressive symptoms over the preceding seven days. The response options are four-point Likert scales, with scores ranging 0-3 and anchor points in terms of the number days per week each symptom was experienced: 'rarely or none of the time (less than one day)' to 'most or all of the time (5-7 days)'. The total score ranges from 0 to 60, with a higher score indicating a higher level of depressive symptoms. The scale has been shown to be reliable and valid in both community and psychiatric samples and a score of 16 or more on the CES-D is generally accepted as an indicative of a clinically significant level of depressive symptoms (10, 11). This cut-off score was used to divide the total sample into high and low depression groups in this study.
The BSI was originally to assess the strength of a person's wishes and plans to commit suicide completed by a clinician using a semi-structured interview (12), modified into a self-report scale with 19 items in Korea (13). The Korean version of the BSI showed acceptable reliability and validity (13). The items are rated on a 3-point scale from 0 to 2. The total score can range from 0 to 38, with higher scores indicating higher suicidal ideation.
The Korean version of STAXI is a self-report scale with 44 items designed to evaluate an individual's anger level. The scale was originally developed by Spielberger (14) and translated into Korean in 1997 (15). Each item is essentially a statement people use to describe their emotions when they feel angry. Each item is assessed by a four point scale (1 = no anger; 4 = maximum anger). The Korean version of the STAXI has been shown to have satisfactory test-retest reliability, internal consistency and validity (15). The score is considered to correlate positively with anger level in subjects.
The BIS was developed by Barrett (16) and is a scale with 23 items selected to measure impulsiveness. This scale has been widely-used as a trait-based, self-report measure of impulsivity. It was translated into the Korean by Lee in 1992, and this version has been found to have adequate reliability and validity (17). Higher scores indicate higher impulsivity.
Statistical analysis
Group differences were tested using either chi-square or Student's t, whichever was appropriate. Partial correlation coefficients were calculated for the correlation analysis. In the stepwise linear regression analysis, the dependent variable was the BSI score and the independent variables were factors known on the basis of past research to be associated with increased risk of suicide (18-20). These were age, gender, level of family income, a family history of psychiatric illness, marital status, education, religious belief, and sleep duration. The data were analyzed using SPSS 15.0 (SPSS Inc, Chicago, IL, USA). Statistical significance was defined as P < 0.05 (two-tailed).
RESULTS
Table 1 summarizes the sociodemographic, psychological characteristics, and sleep durations of total participants. Two hundred ninety four participants (29.4%) showed significant depressive symptom, defined as high CES-D group (≥ 16) as the previous study (9). Participants with the CES-D score less than 16 were classified as low CES-D group (Table 1). Comparisons between the high and low CES-D groups are summarized in Table 1. Compared with the low CES-D group, the high CES-D group was significantly older (mean ages: 41.8 ± 12.0 vs 38.7 ± 11.39, t = -3.814, P < 0.001), had a higher ratio of females (55.4% vs 47.7%, χ2 = 4.933, P = 0.026), were more likely to have a family history of psychiatric disorder (9.9% vs 2.7%, χ2 = 23.369, P < 0.001), were more likely to be married (77.7% vs 71.2%, χ2 = 4.196, P = 0.041), and were more religious (64.6% vs 52.3%, χ2 = 12.862, P < 0.001). The high CES-D group also scored higher on the BSI (6.3 ± 6.5 vs 3.4 ± 3.8, t = -7.148, P < 0.001), the STAXI (38.1 ± 9.0 vs 33.0 ± 7.1, t = -8.648, P < 0.001) and the BIS (64.4 ± 8.7 vs 59.7 ± 9.2, t = -7.634, P < 0.001).
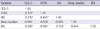
The results of the partial correlation analysis are shown in Table 2. After adjusting for age and gender, the scores on the BSI were found to be positively correlated with the CES-D, STAXI and BIS scores (r = 0.245; P < 0.001, r = 0.344; P < 0.001, and r = 0.152; P < 0.001, respectively). The BSI scores showed no significant correlation with sleep duration on weekday (r = -0.044, P = 0.167).
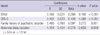
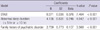
The International Classification of Sleep Disorders (21) defines a 'short sleeper' as someone who sleeps five hours or less a day and a 'long sleeper' as someone sleeping 10 hours or more a day. In the present study, we classified short and long sleepers into an abnormal sleep duration group. The regression analysis revealed that higher scores on the BSI were related with higher scores on the STAXI and on the CES-D, the presence of a family history of psychiatric illness and abnormal sleep duration (Table 3; F = 45.449, adjusted R2 = 0.151, P < 0.001, P < 0.001, P = 0.001, and P = 0.008, respectively). The regression model with high CES-D group showed stronger predictive power, in which higher scores on the BSI were associated with higher scores on the STAXI, an abnormal sleep duration and the presence of a family history of psychiatric illness (Table 4; F = 38.092, adjusted R2 = 0.275, P < 0.001, P < 0.001, and P < 0.001, respectively).
DISCUSSION
This study investigated the relationships between suicide ideation and associated factors in a community population in an urban area of Korea. The results showed that subjective depressive mood, high anger, abnormal sleep duration and a family history of psychiatric illness were related to suicide idea in general population. These relationships were more prominent in the high CES-D group.
The mean CES-D score for the total participants was 11.6 ± 7.3, and 29.4% showed clinically significant levels of depressive symptoms (scores of 16 or higher in CES-D), and this finding is consistent with those reported in previous studies (22). Just as others have done, we proposed the relationship between depression and suicide ideation. From the study done in the past (20), 95% of people who commit suicide have a diagnosis of mental disorder, and 80% of those with a mental disorder are diagnosed as suffering from depression.
In current study, a positive correlation of anger with suicide idea was also found. Previous studies have demonstrated possible relationships between higher anger and suicidality (23, 24). The present study increases our knowledge about the relationship between anger and suicide idea. In Asian culture, the expression of anger tends to be usually discouraged. This represents a major challenge to Koreans who experience anger, but feel pressure to express and manage the emotion in culturally acceptable ways. Lee et al. (23) showed that anger is an important marker for people, who may be at risk of engaging in suicidal behavior. A similar finding was also reported in a Turkish study (24), in which suppressed anger was shown to increase suicidal thoughts. In the present study, intense feelings and tendency to suppress anger might increase suicidal thought.
Previous studies have shown that individuals who suffer from insomnia or sleep disturbance could be at greater risk of depression and committing suicide (25-27). In the current study, we conducted the question on sleep duration which is a feasible additional risk factor for suicide. While many studies have shown that sleep disorders are highly associated with suicide (28-31), no study has been conducted on the association between suicide idea and sleep duration. Looking at the studies of relativity of sleep only commented relation of insomnia or subjective sleep problem and suicide idea done in the past (30-33), it has never used parametric measure of suicidal ideation with scales. In this study, abnormal sleep duration (five hours or less or 10 hr or more) was related with higher suicidal ideation.
There was a study on the association of hypersomnia with suicidality the past (27), but the previous study only focused on the increasing rate of suicides in depressed patients with hypersomnia. To the best of knowledge, this is the first study which showed the relationship between long sleep duration and suicide idea. One possible explanation of this association between long sleep duration and suicide idea is that hypersomnia may be mainly related to depression with atypical features (20). Another possible reason is that hypersomnia or long sleep can be associated with sleep disorders, such as sleep apnea and narcolepsy, which are known to be related to depression (30, 31). Moreover, the finding that sleep disorders such as nightmare's can be related to increased suicidality after controlling for depression (28) suggests that suicide may be directly related to sleep disturbances and not always mediated by depression.
In current study, the presence of a family history of psychiatric illness (within their second-degree relatives) was related to higher suicide idea. Psychiatric patients with history of psychiatric illness in their biological family are known to respond less well to treatment, leading to an unfavorable prognosis (34). A feasible explanation is that this unfavorable treatment response can be related to higher suicidality, and the other interpretation imply that suicide can be significantly controlled by biological and genetic factors. This common notion is supported by a number of research findings suggesting biological mechanisms of suicide such as genetic factors (35, 36). In addition, Roy and Segal (37) found higher rates of concordance for suicidality in monozygotic than in dizygotic twins.
Impulsiveness measured by BIS scores used in the present study, did not predict high suicide ideation. In a past research, impulsiveness has been considered to be one of the important factors associated with suicide (38). One possible explanation for this inconsistency is that we related impulsiveness to suicidal ideation rather than actual attempted suicide. This finding suggests that impulsiveness may be strongly related to suicidal behaviors rather than suicide thoughts. More research is needed before any firm conclusions can be drawn about the relationships between impulsiveness and suicidality.
The present study has several limitations. Firstly, the methodology involved subjects completing self-report questionnaires without structured or semi-structured interviews. This precluded an objective assessment of subject's psychiatric status. Secondly, we relied entirely on measure of sleep duration, which was also self-reported. This made it impossible to identify secondary symptoms of sleep disorders may have been related to suicidal ideation. Thirdly, the present study design was cross-sectional, and hence limits our ability to assess causal associations between suicidal ideation and associated risk factors. Thus longitudinal studies are needed to clarify causality.
In spite of several limitations, the current study is meaningful, because it assessed risk factors for high suicide idea in a general urban population using representative samples randomly recruited from city districts and matched equally in terms of gender and age group.
In conclusion, our results suggest that depressive mood, high anger, short or long sleep duration and a family history of psychiatric illness might be risk factors for suicide idea in the general population. Therefore, mental health professionals might pay special attention not only to one's subjective mood state (including depressiveness and anger), also sleep duration and family history of psychiatric illness to evaluate suicide risk factors in a community.

 XML Download
XML Download