

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
End-stage renal disease (ESRD) is a well-established risk factor for reduced bone mineral density (BMD) and osteoporosis as well as for hip fracture (1-3). Since the relationship between renal function and BMD in ESRD patients has been extensively investigated (4-7), it is suggested that an association between a moderate to severe decrease in glomerular filtration rate (GFR) in the absence of dialysis (K-DOQI [Kidney Disease Outcomes Quality Initiative] 3 and 4) and BMD (or osteoporosis) may exist among the general population (6, 7). Though the values of GFR and BMD vary across ethnicity, most previous studies of the potential association between renal function and BMD among the general population with stage 3 or 4 CKD have been performed in Western countries (6, 7). There have been few studies regarding renal function and BMD among the general population with moderate to severe (stage 3 or 4) chronic kidney disease (MS-CKD) in Korea or Asia. Furthermore, former studies have been performed only in postmenopausal women (8, 9) or with small sample sizes (9).
In addition to ethnicity, previous studies concerning bone health have also been conducted mainly for women, especially postmenopausal women (8-10). Few studies have been performed on men. Given the increasing prevalence of both osteogenesis and CKD without dialysis and osteoporosis in Asian countries (11, 12), even among men, evaluating the relationship between decreased renal function and BMD in both Korean men and women is of great importance. Therefore, we investigate the association between MS-CKD and BMD in the general Korean population.
MATERIALS AND METHODS
Data source and study subjects
The present study used the BMD data subset of the Korean National Health and Nutrition Examination Survey IV (KNHANES IV) of 2008. The KNHANES collected representative data on the health, nutritional status, and BMD of the civilian, non-institutionalized Korean general population. A stratified multistage clustered probability design was used to select representative samples of non-institutionalized Korean civilians for the KNHANES (13). The survey data were publicly available. A total of 3,583 subjects were recruited in the BMD sub-dataset. We excluded the data from individuals that did not include serum creatinine levels (n = 116). The data for BMD and clinical examination findings, including serum creatinine levels, were available for a total of 3,467 individuals. Individuals with incomplete survey responses (n = 8), diagnosis and treatment of osteoporosis (n = 257), or ESRD (eGFR < 15 mL/min/1.73 m2) and dialysis (n = 12) were also excluded, leaving a total of 3,190 subjects.
BMD and definition of osteoporosis
In KNHANES IV, subjects were examined in a mobile examination vehicle. Licensed, trained technicians measured BMD in men and non-pregnant women aged ≥ 20 yr by using dual energy X-ray absorptiometry (DXA; HOLOGIC, DISCOVERY-W, Bedford, MA, USA). BMD was measured at several areas (whole femur, femoral neck and lumbar spine). BMD was expressed as g/cm2. For the purpose of DXA quality control, daily automatic calibration was performed to maintain a precision standard of 1.5% for the total hip measurements according to the manufacturer's instructions (13). Osteoporosis was operationally defined as a T-score of equal or below -2.5. T-score was estimated using the following equation: (measured BMD - mean of maximum BMD)/standard deviation (SD) of maximum BMD. As there is no universal consensus on maximum BMD, an Asian standard (Japanese) measured for BMD was used. The mean (± SD) values in the femur neck were 0.846 (± 0.124) for males and 0.803 (± 0.107) for females. The values in the total femur were 0.940 (± 0.137) for males and 0.851 (± 0.115) for females. The values in the lumbar spine were 1.024 (± 0.120) for males and 1.006 (± 0.115) for females (14).
GFR estimation
In KNHANES IV, serum creatinine was measured using the Jaffe method and a Hitachi Automatic Analyzer 7600 (Hitachi, Tokyo, Japan), and serum creatinine concentrations were calibrated to a creatinine standard. Renal function was estimated using the estimated glomerular filtration rate (eGFR). As Modification of Diet in Renal Disease (MDRD) study population had been derived from almost non-dialysis patients with CKD (15), the GFR of healthy people might be underestimated by the MDRD equation. Therefore, we estimated the GFR (mL/min/1.73 m2) using the following Cockcroft-Gault (CG) formula: eGFR (mL/min/1.73 m2) = ([140-age] × weight × [0.85 if subject was female])/72 × serum creatinine, adjusted for body surface area (BSA). BSA was calculated as follows: BSA = weight (kg)0.425 × height (cm)0.725 × 0.007184 (16). With K-DOQI, MS-CKD was defined as subjects with eGFR < 60 mL/min/1.73 m2 (K-DOQI stage 3 or 4).
Covariate assessments
Body mass index (BMI) was calculated by dividing weight (kg) by square of height (m2). BMI was classified into the following 3 groups: underweight (BMI < 18.5 kg/m2), normal weight (BMI 18.5 kg/m2 to < 25 kg/m2) and obesity (BMI ≥ 25 kg/m2) (13). Daily calcium intake (mg/day) was calculated using the 24-hr recall method. Information concerning cigarette smoking (never smoked & ex-smoker/current smoking), alcohol consumption (less than once per month/more than once per month), exercise (none/1-2 times per week/3-4 times per week/5 times or more per week), and menopause and hormone replacement therapy, and fracture-related history, such as any history of osteoporosis in family members and any history of fracture in themselves (no/yes) were assessed using survey questionnaires.
Statistical analysis
All statistical analyses were performed using SAS software, version 9.2 (SAS Institute Inc, Cary, NC, USA) to account for the stratified multistage clustered probability design and survey weights. The age-standardized prevalence of osteoporosis was measured by using the standardization methods for the population derived from the 2005 Korean Census as the standard population. For continuous variables (age, BMI, daily calcium intake, vitamin D level, and BMD at various sites), a univariate regression analysis was applied to evaluate the difference in means between subjects with and without MS-CKD according to statistical guidelines (13). For categorical variables (BMI, smoking status, exercise, alcohol consumption, fracture-related history, and menopause & hormonal replacement threrapy), a Rao-Scott chi-square analysis was applied to account for differences in terms of the absence or presence of MS-CKD. The relationship between eGFR and BMD was determined in terms of sex by MS-CKD stratified simple and multiple regression analysis (SAS syntax: SURVEYREG); after adjustment for age and BMI, covariates were related to bone health (age, BMI, daily calcium intake, vitamin D level, alcohol consumption, cigarette smoking, exercise, and fracture-related history, as well as menopause and hormone replacement therapy in females). The association between MS-CKD and osteoporosis was estimated using a logistic regression model. For the first step, adjustments were made for age and BMI. Next, multiple logistic regression analysis included all variables. The reference category in each model was an eGFR of ≥ 60 mL/min/1.73 m2.
Ethics statement
The design of the present study was approved by institutional review board of the Catholic University of Korea, College of Medicine (approval ID: CUMC11U139). The Korea Center for Disease Control and Prevention received the informed consent from all participants (13). The data are publicly available in website (13).
RESULTS
The estimated percentages of subjects with MS-CKD were 6.4% in males and 17.0% in females. The subjects with MS-CKD were older than those with an eGFR of ≥ 60 mL/min/1.73 m2. Both males and females with MS-CKD were more likely to have lower BMD and calcium intake. The subjects who were underweight or normal weight, former smokers/non-smokers, and who had a history of fracture risks had higher prevalence of MS-CKD in all four groups. Women with MS-CKD were more likely to be taking hormone replacement therapy (Table 1).
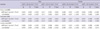
Table 2 shows the association between eGFR (per 5 mL/min/1.73 m2) and BMD. Multiple regression analysis revealed that in both males and females, the BMD at femur neck, total femur, and lumbar spine area were positively associated with eGFR among those with MS-CKD. The regression coefficients of eGFR on BMD were higher in females with MS-CKD (β = 0.013-0.019) at all sites than in those with an eGFR of ≥ 60 mL/min/1.73 m2 (β = 0.007-0.008). For males, the regression coefficients of eGFR on BMD were higher in males with MS-CKD (β = 0.017-0.022) at total femur (P < 0.001) and lumbar spine (P = 0.014) than in those with an eGFR of ≥ 60 mL/min/1.73 m2 (β = 0.010-0.011) (Table 2).
DISCUSSION
Our study results revealed that there was a positive association between eGFR and BMD in the Korean population and that both men and women with MS-CKD were likely to have a higher decline in BMD than those with an eGFR of ≥ 60 mL/min/1.73 m2 in multiple linear regression analysis.
In ESRD patients undergoing dialysis, the bone loss resulted from secondary hyperparathyroidism. However, there have been few reports of obvious mechanisms for the association between BMD and MS-CKD in terms of the degrees of CKD. Recently, some studies have suggested several possible mechanisms behind bone loss in patients with MS-CKD without dialysis (17-19). As GFR decreases below 60 mL/min/1.73 m2, phosphate retention in blood triggers a rise in parathyroid hormone (PTH) and fibroblast growth factor-23 (FGF-23) as well as a decline in tubular 1,25(OH)2 vitamin D; these changes may have a negative influence on BMD (17). Another possible mechanism is that chronic metabolic acidosis characterized by decreased serum bicarbonate may result in a gradual dissolution of bone mineral (18). Consistent with our study results, a study concerning early impairment of bony structures revealed that early trabecular microarchitectures were seen in K-DOQI stages II through IV (20). That study also showed early impairments of bony structures among early stage CKD patients. However, they did not explain why the more severe degrees of CKD had greater bone loss. Therefore, further studies should be conducted to demonstrate a biologically plausible explanation of difference in bone loss between early and severe stage CKD.
There have been few studies concerning the association between BMD and renal function in males. Our study demonstrated that both males and females with MS-CKD had higher ORs for osteoporosis. Consistent with our study results, a prospective study has supported this association (4). In the prospective Osteoporotic Fractures in Men (MrOS) study, a correlation between changes in total hip BMD and the eGFR quartiles (calculated using a MDRD formula) was reported. The mean annualized BMD percentage changes of -0.58%, -0.39%, -0.37%, and -0.31% for the first (lowest) to fourth (highest) eGFR quartiles, respectively (P for linear trend = 0.020) were also shown in multiple regression analysis (4). As this study demonstrated a significant association between eGFR and BMD observed in the males from their cohort, its results suggested that a positive association between eGFR and BMD might exist in males.
Since ethnic differences in bone density and GFR are well described (10, 21, 22), we can assume that the relationship between GFR and BMD may be different among ethnic groups. The effect of height, weight and/or body composition (fat mass, lean body mass, etc.) may result in ethnic differences in bone mass (23). Our study demonstrated that the age-standardized prevalence of osteoporosis in individuals with MS-CKD were lower (9.5% for males and 18.0% for females in Table 3) than those of previous studies in Western countries (6, 24). However, due to the fact that subjects were recruited from a certain hospital in Ireland, there may have been a selection bias in that older subjects or those with more co-morbid diseases related to osteoporosis or kidney disease had been referred to the hospital for DXA and assessments of renal function (24). Environmental factors and lifestyle may also affect ethnic differences in bone density. A previous study has shown that US born Japanese females may have significantly higher body fat and BMD than native Japanese females due to lifestyle differences (25). Thus, ethnic and environmental differences may play an important role in evaluating association between BMD and other factors. Further studies are needed to generalize the association between BMD and MS-CKD in the absence of dialysis in the Korean general population as well as in other ethnic groups.
In our study, serum vitamin D was higher in males with MS-CKD than in those without. Our data was not in accordance with previously described mechanism through vitamin D deficiency (17). After adjustment for potential confounding factors, such as age and smoking, multiple regression analysis was performed (not shown in Tables). Although a positive regression coefficient was found for MS-CKD (2.915; comparing to those with eGFR ≥ 60 mL/min/1.73 m2) and serum vitamin D levels (unadjusted), non significant regression coefficient of MS-CKD (-0.157; comparing to those with eGFR ≥ 60 mL/min/1.73 m2) was also seen after adjustment for age and smoking rate. Therefore, age and smoking rate might serve as confounders for serum vitamin D levels. Furthermore, with the limitation of the KNHANES survey, the authors could not check for supplement use including vitamin D or the active form of vitamin D (including 1,25(OH)2D; calcitriol). Thus, further longitudinal studies are required to confirm this issue.
Our study had some limitations. First, the data were derived from the cross-sectional KNHANES survey, and so we could not evaluate the causal relationship between MS-CKD, BMD and osteoporosis. Second, measurement of GFR with 24-hr urine collection was not available. A 24-hr urine collection is a more precise method for measuring creatinine clearance or GFR than the CG formula and MDRD equation used in research, and this urine collection was used in a previous epidemiological study (26). However, this method is not feasible in the context of population-based studies, such as the KNHANES and the NHANES, which estimated eGFR using serum creatinine instead (6, 7, 9). Third, it was necessary to estimate the figures for patients with a family history of osteoporosis and the number of patients with 'fragility' fractures at the age of > 50 yr. However, due to the limitation of our questionnaire, we could not evaluate this issue.
Our study had some strengths, including the use of a large, healthy and community-based study population. To the best of our knowledge, our study is the first to evaluate the association between MS-CKD, BMD and osteoporosis in the Korean general population. In addition, we performed sex-stratification and age-standardization for the prevalence of MS-CKD as well as adjustments for known confounder, including eGFR and BMD. This point is important because the CG formula uses age, sex, weight and BSA to estimate GFR and because it would be unclear whether the observed association was a consequence of renal dysfunction or confounders, such as age or sex.
In conclusion, the results of present study provide important evidence to support an association between GFR and BMD in both males and females and suggest that osteoporosis may be highly prevalent in individuals with MS-CKD in the Korean general population. Further longitudinal studies are warranted to investigate the potential effects of MS-CKD on individuals from the general population who are vulnerable to osteoporosis. Hence, screening procedures for the early detection of such patients should be established.


 XML Download
XML Download