

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Teratoma is common neoplasm that is typically encountered in infants and children. The majority of cases is benign, and arises from the sacro-coccygeal region, ovary, mediastinum, or retroperitoneum. A small percentage of cases exhibit malignant components, present at unusual site, or present during adult middle age (1). Primary germ cell tumors of the mediastinum represent approximately 10% of all neoplasm in the mediastinal area. The histopathologic features are similar to those of germ cell tumors in the gonads (2, 3). Malignant transformation in mediastinal germ cell tumor, especially to embryonic rhabdomyosarcoma is very rare (4-7). Furthermore, mediastinal embryonal rhabdomyosarcoma that arose from benign mature teratoma without other germ cell tumor components has not been reported in English literature, to our knowledge. In this report, we present such a case of a primary embryonal rhabdomyosarcoma of the anterior mediastinum that arose from a tumor that was only associated with a mature teratoma in middle-aged adult.
CASE DESCRIPTION
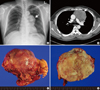
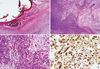
A 46-yr-old man presented with chest trauma as a result of an accident on 10 September 2011. On chest X-ray, an anterior mediastinal mass was detected (Fig. 1A). To obtain further information, chest computed tomography (CT) with contrast enhancement was performed, revealing a 9.5-cm-sized anterior mediastinal mass (Fig. 1B). The initial radiological diagnosis was thymoma. The radiological differential diagnoses were germ cell tumor and mediastinal sarcoma. Clinical and ultrasonography examination of the testicles were normal. Complete surgical excision was performed and entire specimen was evaluated. Grossly, the specimen showed a well-circumscribed 9.5 × 8 × 6-cm-sized round firm mass that was covered with normal thymic and perithymic soft tissue (Fig. 1C). The cut surface was flesh-colored and pale tan appearances (Fig. 1D). Microscopically, tumor demonstrated two different areas, including mature teratoma and sarcomatous area. In the teratoma area, the tumor demonstrated mature squamous epithelium, hair, skin appendage, adipose tissue, and other mesenchymal tissue (Fig. 2A). Immature components were not identified. There is also intermingled areas compact cellular and loose and myxoid area (Fig. 2B). In the sarcomatous area, there is some histological architecture resembled embryonic muscle, which forms aggregates of myoblasts amid loose, myxoid mesodermal tissue. The myoblastic tumor showed sheets of rhabdoid cells, which were small and spindled in appearance, and demonstrated moderate to poor differentiation. The cell also demonstrated deeply eosinophilic cytoplasm, and small eccentric oval-shaped nuclei (Fig. 2C). Immunohistochemical (IHC) analysis revealed a strong positivity to anti-myogenin and anti-desmin antibodies in the rhabdomyosarcoma component (Fig. 2D). The surgical resection margin was clear. After surgical excision, two cycles of dactinomycin-based chemotherapy were performed. Lung metastasis was detected on follow up CT on September 2012, and wedge resection was performed. Pathological finding of lung lesion showed same feature with that of primary rhabdomyosarcoma.
DISCUSSION
In our pathologic examination, sarcomatous area of tumor showed typical histological characteristics of embryonic rhabdomyosarcoma. It showed same typical cellular features with usual embryonal rhabdomyosarcoma. These tumor cells were confirmed by immunohistochemical marker, such as anti-myogenin and anti-desmin antibodies.
A review of literature revealed 32 previous reported patients with mediastinal rhabdomyosarcoma (including all subtypes) that arose from germ cell tumor in 12 separate studies (1-15). The average age of these patients (excluding 2 cases that lacked data) was 26.4 yr. The majority of patients were men (M:F ratio = 28:2). Among these 32 cases, embryonal rhabdomyosarcoma was only observed in 8 cases. Of particular note, there were no reported cases of embryonal rhabdomyosarcoma with only a mature teratoma, thus making our present case unique.
A non-germinal malignant tumor developing within a germ cell tumor is an extremely rare event in both gonadal and extragonadal loci. Moreover, embryonal rhabdomyosarcoma in adult patient's mediastinum is also very rare (4). In our review of the pathological findings reported in the literature, only three studies describe and undetermined type rhabdomyosarcoma with teratoma (1, 14, 15). In all reports, rhabdomyosarcoma was usually observed in combination with seminoma (6), myxoid liposarcoma (4), immature teratoma (4, 9, 13), embryonal carcinoma (4-6, 10), chondrosarcoma (4), choriocarcinoma (5), endodermal sinus tumor (6), angiosarcoma (6), and yolk sac tumor (7, 10, 13) (Table 1). This may represent important histological evidence that rhabdomyosarcoma arises from skeletal component of a mature teratoma. Consistently, previous immunohistochemical studies support this possibility.
In general, the prognosis for patients with mediastinal rhabdomyosarcoma is poor. Possible causes of this are the difficulty in obtaining early detection and the chemo-resistance of these tumors, and proper metastatic potential. The detection diagnosis of mediastinal rhabdomyosarcoma is usually fortuitous. Furthermore, because the common initial radiological diagnosis is benign thymoma, clinicians often pay little attention to these lesions (3). Unfortunately, these tumors exhibit chemo-resistance and metastatic potential (2, 14, 16), and presently, there is no standard schedule for performing chemotherapy to treat adult cases of embryonal rhabdomyosarcomas. Even existed pediatric protocols are often not effective in either the germinal and non-germinal components. Patients die mostly as a result of regional involvement and multiple metastases (4, 10). However, if complete excision is performed, the recurrence rate will decrease (10, 17).
In summary, primary rhabdomyosarcomas arising from mature teratoma in the mediastinum are very rare in adults. Because of the risk of recurrence in these cases, complete surgical resection should be considered both before and after chemotherapy.

 XML Download
XML Download