

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Long-distance road marches are usually conducted in the military to train soldiers (1-4). In Korea, however, a popular civilian event called the 'University Student Grand Voluntary Road March' has been held. College students are allowed to volunteer for participating in this march, and the applicants face a tough competition for selection. The participants are required to walk a long distance (580 km) carrying a certain weight over a long period of time (21 days) to complete the march.
Prolonged road marches have resulted in specific physical problems (1, 3, 5-7). In previous studies, prolonged foot marches were associated with the development of acute injuries such as sprain, blister and other complications which limited daily activities (1-3, 8, 9).
Medical knowledge about the injuries from a strenuous road march can contribute to the reduced incidence rate, early recognition and prompt treatment of such injuries (10-12). To our best knowledge, most previous studies regarding road-march injuries were conducted only in a day. In addition, there are only a few studies that investigated civilian injuries during road march (2, 13-15). Thus, an increased level of details on road-march and related injuries as in our study can be beneficial in terms of medical preparedness, risk assessment, and preventive measures. Such studies can provide useful information applicable to long distance marches, hiking and trekking. Therefore, we investigated types of injuries in single young healthy cohort during the 580 km University Students Grand Voluntary Road March in 2012.
MATERIALS AND METHODS
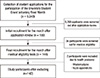
A total of 144 college students who participated in the 15th University Students Grand Voluntary Road March 2012 were included in this study (Fig. 1). In this march, they were required to complete 580 km by walk carrying a certain weight (14.1 ± 1.4 kg) (Fig. 1). In Fig. 2, the selection procedure of research participants is illustrated.
University students grand voluntary road march in Korea
The first University Students Grand Voluntary Road March in Korea was organized by a Korean pharmaceutical company in 1998. Ever since, selected college students have participated in successive annual events under the slogan of "Find your passion in yourself." The participants underwent medical screening before the event. This included blood tests, EKG and spinal X-ray. The 15th annual event was scheduled from July 4th to July 24th, 2012. The average walking speed was expected to be about 29 km per day. The participants were required to march for 8 hr each day. They took 10 to 15 min rest-breaks every hour. The roads were either dry or wet depending on changing weather. The roads were mostly asphalt-paved and typically on a hilly terrain with altitude varying between 50 and 100 meters.
On the first day of the march, each individual's carrying weight was measured. The total weight carried by each participant was 14.1 ± 1.4 kg. This was composed of a backpack (1.0 kg), personal belongings including clothes (7.3 kg), and camping equipment (5.8 ± 2.0 kg).
Medical data
A total of seven medical teams made of 35 staffs performed medical assessment during the road-march. Each team was composed of five staff members including a medical doctor. The medical doctors spent three marching days in turn. The subjects' medical data were collected by way of passive and active monitoring. Passive monitoring was conducted when the subjects with injuries visited medical staff themselves. All the injuries that were confirmed from the monitoring were recorded on a medical record form. The forms were prepared by the medical staff in advance. For passive monitoring, the medical team marched along with the participants, or in an ambulance which followed them. After the road march ended, the medical staff conducted follow-ups for 7 days so as to confirm the development of further injuries. Passive monitoring was conducted in two ways. First, medical staff observed injuries, and then recorded date, type, location, treatment and courses of injuries at a designated service area. Second, medical staff analyzed all the medical data that were collected during the march and classified the injuries that developed due to marching.
Active monitoring was conducted by confirming new and previous injury development in the subjects at the end of each marching day. Through the active monitoring, development of blisters, abrasions, sprains and other injuries were recorded on medical record forms.
In the present study, road-march injuries were overuse damages and traumatic injuries that developed either during the march or the follow-up period. Overuse injuries were skin or skeletomuscular damages caused by repetitive microtraumas, included abrasion blisters, sprains and fatigue bone fractures. Traumatic injuries were acute injuries such as sprain or fracture caused by a single accident, which included falling or colliding with objects. A foot map with assigned number indexes was devised to help assessing foot blister lesions that developed during the march (Fig. 3A). To help assess the pressure and the abrasion level, a shoe map was similarly devised (Fig. 3B).
All the subjects wore their own cotton socks. A new pair of running shoes was provided for them by the event organizer. One day prior to the march, their socks and shoes were checked if they were in good condition.
Questionnaire
All the subjects received a questionnaire and filled it out 15 days before the march. The questionnaire included questions about the respondent's gender, age, dominant hand, and history of military service if any.
Medical screening
The weight and height of the subjects were measured when they were barefoot and wearing only an underwear. Additionally, EKG and lumbar X-ray were obtained.
The authors collected data on gender, age, body weight, hand dominance, date and location of injuries, type of injuries, and shoe wear patterns based on the medical record forms, questionnaires and physical examinations before the march. In some cases, additional information was collected by interviewing the subjects and the medical staffs. It was determined whether the injuries confirmed upon completion of the march were actually caused by marching or not.
Statistical analysis
The data collected from the medical records and road-march medical transcripts were coded for analysis using SPSS 15.0 statistical package (SPSS Inc, Chicago, IL, USA). Continuous variables were marked as mean ± SD or median (interquartile range). To compare the continuous variables, Mann-Whitney test was used. To compare categorical variables, Fisher's exact test was used. Statistical significance was determined as the P value was less than 0.05.
RESULTS
Subject characteristics and medical screening results
Out of 9,940 total applicants who applied for participating in this march, only 180 students were selected through document screening process. Thirty six who failed the medical screening were screened out. Thus, One hundred forty four students were included in the present study. Two participants dropped out of our study, because one had rhabdomyolysis and the other had acute appendicitis during the road march. Finally, 142 were subjected for the present study (Fig. 2). Mean age of the subjects was 22.4 ± 2.2; gender ratio was 1:1; and mean body mass index (BMI) was 21.7 ± 2.4. Fifty-four subjects had a history of military service, and 88 others did not. In terms of hand dominance, 127 had right hand dominance, 6 had left hand dominance, and 9 were ambidextrous. Twelve subjects showed abnormal EKG results; such as sinus dysrhythmia (n = 3), sinus bradycardia (n = 4), right axis deviation (n = 4), and poor R-wave progression (n = 1). Twenty one subjects showed abnormal lumbar X-ray findings; such as scoliosis (n = 6), lumborosacralization (n = 5), lordosis (n = 8), and spondylolysis (n = 2).
March related foot injuries
During period of the road-march, mean temperature was 25.3 ± 4.0℃ and mean humidity was 93.4% ± 5.6%. Mean road-march time was 310 ± 66 min per day.
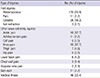
In Table 1, injuries that developed due to the road march are shown. Out of total 142 subjects, 135 (95.1%) suffered from foot injuries. The most common injury was blister and abrasion (95.1%), followed by cellulitis (18.3%), pain (7.7%) and nail extraction (2.1%).
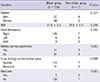
Using the numbering schemes shown in Fig. 3, the initial onset location of blisters on the right foot were location 12 (7%), 16 (7%) and 17 (7%) and 15 (6%). On the left foot, it was at location 45 (10%), 42 (8%), 47 (8%), and 46 (7%). The first blister development was reported on the first day of the road march. On the second day, 51 subjects (37.8%) reported blister development. Dates and locations of the initial blister development are shown in Fig. 4. During period of the road march, the most common location of blisters on the right foot was location 15 (61%), followed by location 16, 14, 22, 25, and 17. On the left foot, location 45 (57%) was followed by location 46, 44, 51, 47, and 52. Results on blister distribution are presented in Fig. 5. In subjects who had reported having blisters developed, more than one blister is confirmed by the medical staff. There was no statistically significant factor between blister group and non-blister group (Table 2).
Injuries in lower extremities other than the foot
The most common injuries other than foot injuries were ankle pain and knee pain, which developed in 18 subjects (12.7%). This was followed by Achilles tendon pain in 11 subjects (7.7%) and thigh pain in 7 subjects (4.9%) (Table 1).
Other concomitant injuries and diseases
Other injuries and diseases included lumbar pain in 6 subjects (4.2%), chest wall pain in 2 subjects (1.4%), and skin rashes in 11 subjects (7.7%). There were also cases of gastrointestinal symptoms such as nausea, vomiting, abdominal pain and diarrhea in 19 subjects, common cold in 12 subjects, meibomian cysts in 2 subjects, cystitis in 1 subject, excessive menstruation in 1 subject and other diseases in 11 subjects.
Observation of shoe bottom
In terms of the right shoe, it turned out that location 10 was worn out the most (89%). This was followed by locations 3, 4, and 2. In terms of the left shoe, location 40 turned out to have been worn out the most (96%), which was followed by locations 33, 34 and 32. The details are depicted in Fig. 6.
Return to daily life
Out of the 142 subjects, 136 subjects returned to their daily lives without medical treatments which lasted for longer than 3 days. However, the rest 6 participants (5 females and 1 male, 4.2%) needed extra medical treatments for longer than 2.5 weeks (IQR: 2 to 3) after they had completed the march to return to their daily lives. Injuries that these participants had were as follows: 1) infected blisters (n = 6), 2) swelling and pain in the ankles (n = 3), 3) swelling and pain in the knees (n = 3).
DISCUSSION
The present study targeted healthy civilians on road-march-related injuries. Previous studies have targeted mainly soldiers. Ours is the first study in this topic investigated injuries associated with road march that was a lot longer in time and distance. Our findings including the common locations of blisters and shoe wear patterns may help in establishing measures for preventing injuries from developing in road march or hiking. During the study period, 135 subjects (95.1%) experienced foot injuries, and 53 (37.3%) experienced injuries that were not foot injuries. Because of injuries associated with the present march, 6 subjects needed extra medical treatments after completion of the march that lasted longer than 2.5 weeks (IQR: 2 to 3) until they returned to their daily lives. One subject had to be treated for 4 more weeks after completion of road march.
A strenuous road march usually results in high incidence rate of injuries (1, 3, 4, 6, 8-10, 16-18). All the injuries in this study were involving the waist or lower extremities. More than half of them were blisters, lumbar pain, and sprains (1, 2, 11, 18-21). In our study, foot injury was the most common injury and developed in 135 subjects (95.1%). The incidence rate was higher than that of previous studies (1, 2). This may be due to extended time period of the march and increased level of humidity (1, 2, 18). Foot blister was the most common. A blister develops due to friction and shear force on the skin (11, 22). Shear force increases mechanical fatigue of the skin epithelia. Consequently, the connections between the cell layers break (11, 23, 24). Blister development was the most common at locations 12 and 15 on the left foot, and at locations 42 and 45 on the right foot. This could mean that the locations subject to most friction and shear had been the 2nd and 5th toes, where most blisters were observed. It turned out that left/right-hand dominance did not have any influence on the blister location. Of the 142 subjects, 3 had left hand dominance, and this result was not statistically significant in terms of blister location. Considering that there were only a small number of subjects who had left hand dominance, further study will be necessary in evaluating the relation between hand dominance and blister location. Initial blister development was reported on the first day of the march, and the highest developments were reported on the second day. These results mostly coincide with those in Reynolds et al. (2). Foot blisters may seem to be a simple problem. Still, according to Knapik et al. (1) about 4% of the soldiers in their study could not finish the road march, and another 4% took a sick leave after they completed the march. In the present study, no subject officially quit marching because of blisters, but blisters can cause discontinuation of marching or difficulty in returning to daily life. Six subjects (4.2%) among those who had sustained blisters or other injuries repeatedly during the period of road march needed extra medical treatments after completion of the march for longer than 2.5 weeks (IQR 2 to 3) before returning to their daily lives. Therefore, we believe that active intervention is essential to prevent the injuries associated with the road march. Since blisters can limit daily activities, development of active prevention or intervention programs are suggested. Examples may include intermittent resting schedule for potential victims, physical massage on the areas of blister precursor and on the joints such as ankles and knees, and early detection strategies of potential victims from thorough and frequent medical discretion. Considering that blisters develop due to repetitive friction and shear forces, massage and physiotherapy treatments may be helpful at location 12, 16, 17, and 15 on the right foot, and location 45, 42, 47, and 46 on the left foot. Additional studies on the treatment of blisters are needed in the future.
In previous studies, a risk factor of blisters was absence of experience in road march (8, 17). In the present study, however, there was no significant difference in terms of blister incidence between the group with long-distance march experience (subjects with history of military service) and the no experience group (subjects with no history of military service). Gender did not affect blister incidence either. Accordingly, we think that the most important risk factor of blister development is the distance and duration of road march. A heavy load has been known as another risk factor of blister development. According to Coopers (25), participants in a 56 km nightly road march carried an 11 kg of load mass, and 43% of them developed blisters. According to Knapiks (1), out of the 180 infantry soldiers who participated in a 20 km road march carrying a load mass of 46 kg, 124 (68.9%) developed blisters. This incidence rate is much higher than that of Coopers (25). Greater the load mass, greater the shear force on the foot, which will increase blister incidence. In this study, average load mass was 14.1 ± 1.4 kg, and 135 subjects (95.1%) reported blister development. Time duration and distance of road march of our study was much longer than those of the previous studies, so it is difficult to comment on the load mass effect on the blister incidence based on our findings.
The subjects were provided with a pair of brand-new running shoes before the march. Fig. 6A shows a diagram of shoe bottoms taken upon completion of the march. We consider this figure to be important in the present study, since it clarifies the locations where the friction and shear forces must have been acting on. Location 3, 4, 9, and 10 were confirmed to have been worn the most on the right shoe, while location 33, 40, 32, and 34 on the left shoe. One can see that the forces were transferred mostly to the lateral sides of the feet during walking, which consequently caused blisters to develop mostly on the 5th toes. Blister incidence may reduce when those parts of the shoes are reinforced or designed to reduce friction. Number, type, and composition of the socks worn may affect blister development as well (7, 26).
In terms of the injuries that are not foot injuries, 36 subjects (25.4%) reported ankle and knee pain. We consider this to be directly related with the prolongation of the foot march. Eleven subjects (7.7%) reported Achilles tendon pain, which had been reported previously in running (13). Achilles tendon pain may be caused by overuse of the tendon and friction against the posterior and medial sides of the shoes. In addition, the prolonged foot march resulted in damages in ankle and knee joints as well as in the Achilles tendon. Massaging the Achilles tendon daily after marching may reduce the injury incidence. Future study is necessary on this topic.
The incidence of lumbar pain or sprain was lower (6 subjects, 4.2%) in this study compared to that in previous studies (1, 2, 9). This might have been due to the lighter load mass in this study compared to those in previous studies (e.g. 14.1 ± 1.4 vs 20 ± 3 kg). In this study, the difference of blister incidence between the two groups with normal radiographic findings and abnormal findings was insignificant. There was no one who quit marching due to lumbar pain. Lumbar pain did not deter the participants from completing road marches in our study just like the results of previous studies.
Limitations of this study are as follows. First, as described above, a total of 7 teams with 35 members including 7 medical doctors performed the assessments and due treatments during the period of road march. All the medical assessments of the injuries were performed by one medical staff in each team. Even though an injury was defined in this study, not all the assessments of the injuries were performed by a single medical staff, so accuracy of the assessments might have been compromised. Second, we were not able to identify the duration of treatment for blisters clearly. Blisters occurred repeatedly in similar areas of the foot and were relatively small. Third, the new shoes that were given to the participants were not checked for the fit. If the shoes did not fit, friction may have increased. We did not identify the characteristics of the socks in the present study, although it could be an important factor influencing blister development. We just knew that most participants wore cotton socks during the period of the march. Fourth, blister and injury incidences might have been affected by elevated humidity level as high as 93.4% on the average. It also rained frequently during the road marching period. Fifth, we do not clarify from left to right when it comes to non-foot injuries. We strongly believe that this piece of information will be needed to clarify the relation between hand dominance and injury types.
In summary, a high incidence rate (95.1%) of injuries was observed in association with this strenuous long-distance road march. These injuries posed an obstacle against the completion of road march and against returning to daily life. Active preventive interventions such as physical therapy and customized reinforced shoes and education program are recommended for reducing incidence rate and severity of injuries.





 XML Download
XML Download