

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Iodinated X-ray contrast media are the most commonly used drugs in diagnostic and interventional procedures. Procedures that employ contrast media have shown rapid growth. In the last two decades, the use of computed tomography (CT) increased by 800% and the use of cardiac catheterization increased by 390% (1, 2). With the increasing use of these procedures, the number of patients receiving iodinated contrast media has also continued to increase. Given such widespread use, it is important to be aware of associated adverse events (AEs) and have a good knowledge about the management of various contrast media.
Most AEs of iodinated contrast media, such as nausea, vomiting, urticaria and itching, are mild. However, severe AEs can occur, including hypotensive shock, respiratory arrest, cardiac arrest and convulsions. The incidence of these AEs has decreased considerably with the change of usage from high-osmolar contrast media (HOCM) to low-osmolar contrast media (LOCM); the incidence of AEs has been reported as 5% to 15% for HOCM and 0.2% to 0.7% for LOCM (3, 4). Although the overall incidence of AEs has decreased, severe AEs still continue to occur. Recently, many different kinds of iodinated contrast media have been used. However, it is not clear whether differences exist in AEs among various LOCM (including iso-osmolar contrast media) (5). Also, it is controversial whether iso-osmolar media are safer than LOCM on the topic of risk for contrast-induced nephropathy. Previous studies have evaluated various LOCM versus an iso-osmolar media iodixanol, but have shown conflicting results (6-8). Therefore, it is important to assess whether the risks associated with these media are class-specific, osmolality based, or individual medium-specific. Different iodinated contrast media may have different biological characteristics. In fact, knowledge of different safety profiles of individual iodinated contrast media is essential.
Spontaneous reporting systems (SRSs) are database resources encompassing reports of suspected adverse drug reactions (ADRs). The availability of real-world data from SRSs provides a rich opportunity to detect post-marketing AEs that are novel in terms of their clinical nature, severity, or frequency since they include populations that are not well represented in clinical trials (9).
Therefore, the objectives of this study were to determine the characteristic AEs of iodinated contrast media and to compare the safety profiles of different iodinated contrast media using data from spontaneous post-marketing AE reports submitted by healthcare professionals of Korean Regional Pharmacovigilance Centers.
MATERIALS AND METHODS
Data source
This study used the database of spontaneous reports of AEs from 15 Regional Pharmacovigilance Centers, including Yonsei University Sevrance Hospital, The Catholic University of Korea Seoul St. Mary's Hospital, Seoul National University Hospital, Asan Medical Center, Dongguk University Ilsan Hospital, Ajou University Hospital, Hallym University Sacred Heart Hospital, Chungbuk National University Hospital, Dankook University Hospital, Keimyung University Dongsan Medical Center, Kyongpook National University Hospital, Inje University Pusan Paik Hospital, Pusan National University Hospital, Chuncheon Sacred Heart Hospital, and Chonnam National University Hospital, in Korea. The ADR reporting system was developed in Korea in 1988 (10). Three Regional Pharmacovigilance Centers were established in 2006 to support the surveillance system and activate spontaneous reports. The initial 3 centers extended to 6 centers in 2007, 9 centers in 2008 and 15 centers in 2009. Since June 2009, the centers have been operating within the framework of the PharmacoVigilance Research Network (PVNet) of the Korea Food and Drug Administration (KFDA) and have been the main contributors to the Korean SRS in recent years. Using the standard operating protocol of PVNet, pharmacovigilance professionals (primarily physicians and pharmacists) collect information on cases of suspected ADR and review them for possible drug causality. Reports submitted by healthcare professionals of regional centers on standardized forms are stored in the national KFDA database (11).
We obtained all reports of ADRs submitted to the KFDA from the 15 Regional Pharmacovigilance Centers between June 24, 2009 and December 31, 2010. Each report contains information on patient demographics, suspected drugs and concomitant drugs, AEs, patient outcomes, results of causality assessment, and report centers. Verbatim drug names supplied in the KFDA data were coded to extract standardized generic names according to the Anatomical Therapeutic Chemical (ATC) classification. AEs were coded using the World Health Organization-Adverse Reaction Terminology (WHO-ART) coding dictionary (12). Results of causality assessment for each AE by the WHO criteria were recorded by the reporters in the database.
AEs of iodinated contrast media
All reports with low-osmolar and iso-osmolar iodinated contrast media (ATC code V08AB) listed as either a suspected or a concomitant medication were identified. Iodinated contrast media in the database were classified as low-osmolar and iso-osmolar. AEs were identified by the WHO-ART Preferred Terms. A report was defined as a serious report if at least one serious AE was present among all the AEs in the report. Serious AE is defined as either of the following: 1) serious outcome (death, life-threatening event, inpatient hospitalization or prolongation of existing hospitalization, persistent or significant disability/incapacity, congenital anomaly/birth defect, and others of medical significance) (13); or 2) the WHO-ART critical term (e.g. anaphylactic shock, angioedema, etc.) (12).
Statistical analysis
A report can contain more than one suspected drug, or more than one AE. We identified a drug-AE pair as a unique combination of a single drug and a single AE. For example, a report containing two AEs with one contrast medium counted as two medium-AE combinations. For the analysis, 2 levels of dataset were used: reports and medium-AE combinations. We analyzed the data at the level of reports; patient demographics (age, gender) and the presence of serious AEs were analyzed; and the number of total and serious reports for each contrast medium was counted. The frequency of AEs was analyzed at the level of contrast medium and AE combinations; the most commonly reported AEs were listed; the most commonly reported AEs were also listed for LOCM and iso-osmolar media, respectively; frequently reported medium and AE combinations were studied.
The safety profile was characterized and compared between LOCM and iso-osmolar media, and between each of the iodinated contrast media. For this analysis, AEs were grouped together as the primary System Organ Class (SOC) in the WHO-ART. The frequency of AEs at the SOC level was then calculated. The chi-square test was used to assess the differences in the frequency of AEs at the SOC level between low-osmolar and iso-osmolar media, and between individual media. A P value of 0.01 was used as the level of significance.
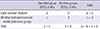
Proportional reporting ratio (PRR) was also calculated to compare the safety profiles of different iodinated contrast media. The PRR is calculated in a similar way to a relative risk in a cohort study, whereby the proportion of specified group (SOC) of AEs is calculated for each medium and divided by the proportion of these AEs for the other iodinated contrast media in the database (reference group) (Table 1) (14, 15). A threshold of lower 95% confidence limit (95% LCI) of the PRRs greater than 1 was used to define the signal of disproportionate reporting between a medium and an event at the SOC level (16). Signals having a mean of the PRR and its 95% LCI of 15 or greater were categorized as high priority for further medical evaluation (17). A prioritizing signal was also defined as a medium-AE combination with the terms of 'rhabdomyolysis', 'agranulocytosis', 'Stevens-Johnson syndrome' or 'toxic epidermal necrolysis', which are more likely to be drug related than others (18). Detected signals were reviewed to identify previously unlabeled AEs. Due to the close attention to contrast induced nephropathy (19), an additional analysis was performed for renal AEs. In this analysis, AEs were classified into two groups: renal AEs and non-renal AEs. Renal AEs were defined as AEs that combined several preferred terms, including 'anuria', 'creatinine clearance decreased', 'nephropathy toxic', 'nephrosis', 'oliguria', 'renal failure acute', 'renal function abnormal', 'renal tubular disorder', 'renal tubular necrosis', 'azotaemia', 'renal failure chronic', and 'renal failure aggravation of chronic'. Two-by-two tables were created for each medium and compared with renal AEs and non-renal AEs for that media in each column. PRR and its 95% LCI were calculated in this table. All statistical analyses were performed using SAS software Version 9.2 (SAS Institute Inc., Cary, NC, USA).
RESULTS
A total of 48,261 reports and 153,557 medium-AE combinations from the database were used between the specified dates. Of these, 6,524 (13.5%) reports were of low-osmolar or iso-osmolar contrast media. The patients had a mean age of 53.2 yr (standard deviation, 12.8). There were 3,361 (51.5%) males, 3,127 (47.9%) females and 36 (0.6%) patients without gender information. Life-threatening events were reported in 12 cases; inpatient hospitalization or prolongation of existing hospitalization was found in 70 cases. The number of patients who experienced AEs of WHO-ART critical terms was 374 (5.7%) (Table 2).
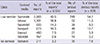
Iopromide (45.5%) was the most commonly implicated iodinated contrast medium, followed by iohexol (16.9%), iopamidol (14.3%) and iomeprol (10.3%). The percentage of serious reports associated with each medium were as follows: for iopromide, 54.2%; iohexol, 11.3%; iopamidol, 8.5%; iomeprol, 10.7%; ioversol, 5.9%; iobitridol, 2.2%; and iodixanol, 7.6% (Table 3).
Of a total of 10,287 medium-AE combinations, the most often reported AEs were urticaria (35.0%), pruritus (26.6%), rhinitis (5.9%), rash (5.8%), and vomiting (2.9%). Among the 603 medium and serious AE combinations, the most frequently reported serious AEs were angioedema (23.6%), face oedema (10.8%), dyspnoea (8.3%), anaphylactic reaction (7.8%), and hypotension (5.8%). The 5 most commonly reported AEs in the low-osmolar media group were urticaria (35.7%), pruritus (26.9%), rhinitis (6.1%), rash (5.2%), and vomiting (2.9%). Those in the iso-osmolar media group were rash (22.9%), azotaemia (19.3%), pruritus (17.3%), urticaria (15.5%), and face oedema (3.0%). The most frequently reported medium-AE combinations were iopromide-urticaria (16.6%), iopromide-pruritus (11.0%), and iohexol-urticaria (6.2%). The most frequently reported medium-serious AE combinations were iopromide-angioedema (12.1%), iopromide-anaphylactic reaction (5.6%), and iopromide-face oedema (5.3%).
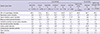
Table 4 presents a safety profile of the iodinated contrast media according to the SOC, by each medium. A statistically significant difference in the frequency of AEs at the SOC level was observed between the low-osmolar and iso-osmolar media groups: the percentage of AEs of 'skin and appendages disorders' was 69.8% and 60.1% (P<0.001); the percentage of AEs of 'respiratory system disorders' was 9.1% and 3.6% (P<0.001); the percentage of AEs of 'central & peripheral nervous system disorders' was 4.2% and 1.2% (P=0.006); the percentage of AEs of 'vascular (extracardiac) disorders' was 1.9% and 0.6% (P<0.001); and the percentage of AEs of 'urinary system disorders' was 1.1% and 24.4% (P<0.001) in the low-osmolar and iso-osmolar media group, respectively. Differences in the AE profiles between individual media were also observed. For iopromide, the percentage of AEs of 'cardiovascular disorders, general' was significantly higher (P=0.001); for iohexol, the percentage of AEs of 'body as a whole-general disorders' was significantly higher (P=0.006); for iopamidol, the percentage of AEs of 'respiratory system disorders' and 'vision disorders' was significantly higher (P<0.001, P=0.009); for iomeprol, the percentage of AEs of 'skin and appendages disorders' was significantly higher (P<0.001); for ioversol, the percentage of AEs of 'gastro-intestinal system disorders' and 'cardiovascular disorders, general' was significantly higher (P=0.002, P=0.008); for iobitridol, the percentage of AEs of 'gastro-intestinal system disorders' was significantly higher (P<0.001); and for iodixanol, the percentage of AEs of 'urinary system disorders' was significantly higher (P<0.001).
Of the 19 signals of disproportionate reporting, 2 were categorized as high priority for further investigation: 'Platelet, bleeding & clotting disorders' (PRR, 29.6) and 'urinary system disorders' (PRR, 22.3) were more frequently reported for iodixanol (Table 5). The AEs, in preferred terms, that are included in the SOC of signals are shown in Table 6. For the signal of iodixanol and 'platelet, bleeding & clotting disorders', the number of medium-AE combinations was 1 as 'purpura'. The patient was male and 62 yr old; he used iodixanol (652 mg/mL) without other concomitant medication and developed purpura with rash. For the signal of iodixanol and 'urinary system disorders', the number of medium-AE combinations was 82 including 65 'azotaemia'; three cases were either experienced inpatient hospitalization or prolongation of existing hospitalization due to AEs. There was only 1 case of Stevens-Johnson syndrome associated with iopromide (labeled AE). In the further analysis for comparison of renal AEs and non-renal AEs, iodixanol was more frequently reported than the other contrast media, with the PRR value of 37.3 (95% CI, 26.6-52.3).
DISCUSSION
This study shows the AE profiles of various iodinated contrast media: iopromide, iohexol, iopamidol, iomeprol, ioversol, iobitridol and iodixanol. Moreover, this study identified the differences in the AE profiles of iodinated contrast media by organ class between individual media. 'Platelet, bleeding & clotting disorders' and 'urinary system disorders' are more frequently reported for iodixanol.
Iodinated contrast media were the suspected drugs reported for comprising great proportions in the database of AEs from the Korean Regional Pharmacovigilance Centers. An increase in patient exposure as well as familiarity with AEs to contrast media by healthcare providers can be explained as a result of pharmacovigilance training by the centers. In Korea, known AEs should be reported along with previously unknown AEs. This was reflected in the results which showed that most centers most often reported known AEs of media (e.g. iopromide-urticaria).
Iopromide was the most frequently reported medium, followed by iohexol. These findings need to be interpreted in light of the consumption data; iopromide (38.8%) and iohexol (18.4%) were the predominantly used iodinated contrast media according to the market share of each medium from the Intercontinental Marketing Services (IMS) KOREA data in 2009 (20). For iopromide and iodixanol, the proportions of each medium among serious reports were higher than those among all reports. This should be interpreted with caution, as difference in the proportion does not suggest difference in the incidence rate of serious AEs.
Frequently reported AEs included urticaria, pruritus, angioedema, hypotension, vomiting, and dyspnea; they appeared to fall under the umbrella of allergic reactions. This was an expected finding because allergic reactions have commonly occurred in patients receiving iodinated contrast media (21).
A significant difference in the AE profiles between low-osmolar and iso-osmolar media was observed. Although LOCM have very similar molecular structures, the individual media have different safety profiles. Gomi et al. (22) found that the proportion of patients experiencing AE varied by LOCM (iomeprol, 3.9%; iopamidol, 2.2%; iohexol, 2.0%; iopromide, 3.5%; ioversol, 1.8%; and all five combined, 2.7%) among the 8,931 patients who underwent contrast-enhanced CT. However, to our knowledge, this is the first study specifically designed to compare the frequency of AEs of iodinated contrast media by organ class between individual media, as well as between low-osmolar and iso-osmolar media.
The frequency of AEs of 'urinary system disorders' was significantly higher for iodixanol and the same was observed for renal AEs. We cannot exclude the possibility that iodixanol, a recommended medium by some guidelines (23), is more frequently used in patients with underlying renal diseases. However, there is still much controversy regarding the nephrotoxicity of iodixanol compared with that of LOCM (24). Nephrotoxicity of contrast media is the third leading cause of acute renal failure in hospitalized patients (25). This difference between iodixanol and the other iodinated contrast media should be considered when selecting a medium among various iodinated contrast media and when monitoring patients during and after its use.
In addition, PRR points to the relative frequency of 'platelet, bleeding & clotting disorders' for iodixanol, including purpura. Contrast media are known to cause some alterations in vascular endothelial function and in platelet function although these effects are not thought to be clinically relevant (26). These effects are related to purpura, however, it is not listed in product labeling. These findings may require continued monitoring.
A measure of disproportionality chosen for this analysis was PRR which cannot be calculated if denominator is zero. Only combination of ioversol and 'red blood cell disorders' were additionally generated signal with information component (IC) of Bayesian Confidence Propagation Neural Network analysis, even though IC can be calculated in all situation (16).
The strengths of this study include the following. First, all reported AEs are identified and reviewed by the healthcare professionals of Regional Pharmacovigilance Centers. The data are more valid than data reported by other reporting sources, e.g., consumers, manufacturers, etc. (27). Second, this study included diverse contrast media: six different LOCM and one iso-osmolar medium, allowing a comparative study of AE profiles; the present study provides better knowledge of the differences between each iodinated contrast medium. Third, since nephrotoxicity of contrast media have been gaining particular interest, the study performed further evaluation for renal AEs by grouping the related terms together.
However, our results should be interpreted in the context of several limitations. First, the lack of information on the denominator, number of patients exposed to each contrast medium, should be considered. It is difficult to assess the relative risk between different contrast media in this study because their incidence rates cannot be estimated. Second, data may have been affected by under-reporting. However, a comparison of the benefit-risk profiles of drugs using this data within the same therapeutic class is generally acceptable (28, 29). In these conditions, the under-reporting can be assumed to be more or less of the same magnitude for the compared drugs (29, 30). Therefore, under-reporting, regardless of its magnitude, does not affect the validity of the conclusions drawn from this study.
In conclusion, the results of this study suggest that the safety profiles of individual iodinated contrast media are significantly different. Particular attention should be paid to the comparative safety evaluation of these media. A better understanding of safety profiles is required to ensure optimum usage and patient safety. This study promotes awareness of diverse iodinated contrast media-related safety signals. Development of criteria for the most appropriate selection of contrast medium among various iodinated contrast media is needed.



 XML Download
XML Download