

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gastroesophageal variceal hemorrhage is the most serious life threatening complication of portal hypertension. In the pediatric population, many underlying diseases cause portal hypertension and esophageal variceal bleeding (1-4). These diseases can be classified into intrahepatic and extrahepatic diseases. Biliary atresia is the most common cause of liver cirrhosis in children. Patients with biliary atresia should undergo a Kasai operation as soon as possible after diagnosis. Of patients with biliary atresia, half of patients will die or require liver transplantation within 6 yr following Kasai operation if the patient first presented with esophageal variceal bleedings (5).
Treatments for esophageal variceal bleedings include pharmacologic, endoscopic and surgical therapies. Endoscopic variceal ligation (EVL) with pharmacologic treatment, including nonselective β-blockers and/or mononitrate isosorbide, is recommended as the treatment of choice to prevent episodes of rebleeding in adults with esophageal varices (6-11).
Although EVL is the most well-studied treatment approach for children with esophageal variceal bleeding (12-14), there are few reports about long-term results of the use of EVL for prevention of variceal rebleeding episodes (12, 15). We focused on analyzing the long-term effects of EVL to prevent variceal rebleeding episodes or the recurrence of varices during a follow-up period of more than 3 yr post-eradication, especially for high-risk esophageal varices.
MATERIALS AND METHODS
Sixty eight children were admitted to Seoul National University Children's Hospital over a 10-yr period due to esophageal variceal bleeding caused by various intra- and extrahepatic diseases. A total of 324 sessions of endoscopic variceal ligation (EVL) were performed to treat variceal bleeding or to prevent rebleeding from esophageal varices in the 68 patients.
Out of the 68 children, 37 were seen for follow-up over a period longer than 3 yr after variceal eradication. These 37 children were included in the study. The mean age at the first EVL was 8.7±4.3 yr (mean±2SD). The study group included 24 male children and 13 female children. The mean duration of follow up after esophageal variceal eradication was 6.4±1.9 yr.
Somatostatin was administered in most patients and blood transfusion was occasionally performed. When patients were hemodynamically stable, the first EVL was performed and the following EVLs were scheduled. Using an endoscope and Stiegmann-Goff endoscopic ligator, all variceal ligations were performed under the general anesthesia. Overtube was not utilized for any patients.
We retrospectively gathered clinical information, endoscopic findings and the results of variceal ligation. Endoscopic severity of esophageal varices was graded either I, II or III (16). Grade I varices are flattened by air insufflation. Grade II varices are not flattened by air insufflation and are separated by areas of healthy mucosa. Grade III varices are confluent and not flattened by insufflations. Other findings associated with a high risk of gastrointestinal bleeding were noted, including the presence of red wale markings on the esophageal mucosa and portal hypertensive gastropathy.
Esophageal varices were defined as eradicated if they were reduced in size to Grade I or were not apparent upon endoscopic examination after EVL. Rebleeding episodes were defined as bleeds that developed after eradication of esophageal varices. Recurrence of varices was defined as varices that newly developed after eradication of esophageal varices. Both the treatment effect of EVL for acute esophageal variceal bleeding and rebleeding rate after variceal eradication were analyzed (17, 18).
This study was reviewed and approved by the institutional review board of Seoul National University Hospital (IRB No. 1307-095-505). We received written informed consent from the parents of all participating children.
The data were analyzed using the SPSS 18.0 software program (SPSS Inc., Chicago, IL, USA). The difference between EVL procedure configurations for intra- and extrahepatic disease was compared using Student's t-test. A paired t-test was used to analyze the efficacy of secondary prophylaxis with EVL, examining the difference between findings before the first EVL and after eradication of esophageal varices.
RESULTS
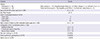
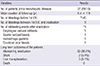
The underlying diseases of 37 patients was classified into intra- (n=19) and extrahepatic (n=18) diseases. Biliary atresia (n=14) and portal vein thrombosis (n=16) were the most common causes of intra- and extraheptic diseases, respectively (Table 1). At the time of first EVL, there were no patients with grade I esophageal varices, 15 patients with grade II and 22 patients with grade III. To attain eradication of esophageal varices, the mean numbers of EVL sessions and of O-bands per session required were 1.9±1.2 and 3.8±1.5 , respectively. The mean interbanding interval to eradication was 1.2 months between sessions. Red wale markings and portal hypertensive gastropathy were detected on the first EVL in 23 (62%) and 23 (62%) patients, respectively. Gastric varices were noted during the first EVL treatment in 9 patients (24%).
The efficacy of secondary prophylaxis with EVL was analyzed (Table 2). The mean duration of follow-up after eradication was 6.4±1.9 yr. Before the first EVL, 145 bleeding episodes occurred in 37 children. However, after eradication of esophageal varices, only 4 episodes of rebleeding occurred in 4 out of 37 patients (P=0.000). The four rebleeding episodes included an esophageal variceal bleed, a gastric variceal bleed, one episode of hemorrhagic gastritis and a duodenal ulcer bleed. There was no significant difference in the frequency of rebleeding episodes between patients with intra- or extrahepatic disease. Only one (2.7%) of 37 patients presented with recurrent esophageal varices after eradication.
A few patients presented with minor chest pain or abdominal discomfort immediately after EVL. EVL-related bleedings were rare and minor. With regards to the long-term prognosis of the study patients, 31 patients (83.8%) maintained eradication status (Table 2). Two patients with portal vein thrombosis (5.4%) had distal splenorenal shunts due to gastric varices and pancytopenia, respectively. Three patients (8.1%), consisting of 2 patients with biliary atresia and 1 with Wilson's disease, underwent liver transplantation due to disease progression of liver cirrhosis. No deaths occurred.
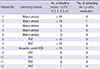
We also identified a prominent decrease in the frequency of bleeding before and after variceal eradication in 12 children who each had more than 5 bleeding episodes prior to the first EVL treatment (Table 3).
DISCUSSION
We analyzed the long-term results and the efficacy of secondary prophylaxis in children with high-risk esophageal varices. The mean duration of follow up after esophageal variceal eradication was 6.4±1.9 yr. Our study included many patients with high-risk esophageal varices, including 23 out of 37 patients (62%) noted to have red wale markings at the initial endoscopy. For the 37 pediatric patients in the study, a total of 145 episodes of esophageal variceal bleedings was noted before the first EVL treatments, reduced to 4 rebleeding episodes after eradication. Recurrence of esophageal varices occurred in 1 out of 37 children. We also identified a prominent decrease in the frequency of bleeding before and after variceal eradication in 12 children who each had more than 5 bleeding episodes prior to the first EVL treatment.
There are few reports regarding the effect of secondary prophylaxis for long-term periods after eradication (12, 15). Duche et al. (15) reported the efficacy of EVL to prevent rebleeding episodes, but the mean duration of follow-up was 28 months (range 1-128). In their study, rebleeding episodes after eradication developed in 2 out of 22 patients. Dos Santos et al. (12) reported a high rate of rebleeding episodes (27.8%) and a high rate of recurrence of esophageal varices (44.4%) in the EVL-alone group, over an average follow-up period of 4.2 yr after eradication.
We performed EVLs at a mean interval of 1.2 months. The initial sessions were spaced more closely (monthly) and once control of bleeding had been achieved were given more infrequently (every 3-6 months) until the varices were eradicated. Although many authors had recommended performing EVL treatments every 1-3 week (19-22), Harewood et al. (23) revealed the interval was significantly shorter in the rebleeding group (2 weeks; interquartile range 0-2 weeks) than in the non-rebleeding group (5 weeks; interquartile range 3-7 weeks) of adult patients with esophageal varices.
We did not use pharmacologic treatments, such as propranolol, nadolol and mononitrate isosorbide, for secondary prophylaxis. According to adult guidelines (9, 10, 24, 25), EVLs with nonselective β-blockers and/or mononitrate isosorbide is recommended as the first choice for secondary prophylaxis in adults with esophageal variceal bleeding. In contrast to adults, children with variceal bleeding have poorer outcomes after EVL with pharmacologic treatment when compared to EVL alone (12). Propranolol prophylaxis avoids the risk of endoscopic treatment. However, the risks of variceal bleeding and mortality increase when propranolol is discontinued (26). In children, propranolol is not recommended for routine use at this time because of insufficient data on its safety and efficacy (27).
Over long-term follow-up of the study patients, there were no deaths. Two (5.4%) and 3 (8.1%) patients underwent distal splenorenal shunt and liver transplantation, respectively. Dos Santos et al. (12) and Duche et al. (15) reported a mortality rate of 9% during long-term follow-up after eradication of esophageal varices in children with esophageal variceal bleeding.
In conclusion, over long-term follow up after esophageal variceal eradication using EVL alone in children with esophageal variceal bleeds, rebleeding episodes and recurrence of esophageal varices were rare. EVL is a safe and highly effective method for the long-term prophylaxis of variceal rebleeding in children with portal hypertension.
 XML Download
XML Download