

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Occupational asthma (OA) is characterized by variable airway obstruction and bronchial hyperresponsiveness attributable to a particular work environment. It accounts for up to 15% of all cases of adult-onset asthma (1). Isocyanate, reactive dyes, heavy metals including nickel (Ni), chromium, cobalt and platinum, and grain dust are frequently reported agents of OA in Korea (2).
Polyvinyl chloride (PVC) is a polymerized form of vinyl chloride, which is extensively used in the plastics industry and in manufacture of synthetic leather, wallpapers, floor coverings and electric cable sheaths (3). Several studies have reported that inhalation of vinyl chloride increases the risk of cancer and pulmonary fibrosis (4, 5). Irritative respiratory symptoms and meat wrappers' asthma syndrome are generally thought to be related to PVC decomposition products, such as hydrochloric acid and/or phosgene, but not to PVC itself.
To date, a few cases of OA induced directly by PVC dust exposure have been reported among workers in meat processing factories and those involved in manufacture of plastic seals (3, 6, 7). The case presented here is, to our knowledge, the first case of OA confirmed by bronchoprovocation tests with both PVC and Ni, and increased airway inflammation after challenge.
CASE DESCRIPTION
A 34-yr-old male had been employed for 7 months at a wallpaper manufacturing factory immediately after moving from the roller processing industry. He had suffered from a cough and chest tightness after engaging in mixing PVC dust into plasticizers and pulverized stone powder for 4 months. When he visited the emergency room with dyspnea in October 2011, he was diagnosed with an acute asthma attack based on wheezing, a forced expiratory volume in one second (FEV1) value that was 74% of the predicted value and 90% sputum eosinophils. He had no relevant medical history or family history of allergic diseases. Chest X-ray showed no abnormalities. Blood tests revealed a WBC count of 8,200/µL (neutrophils 61.1%, lymphocytes 27.6%, eosinophils 4.4%) and a hemoglobin level of 14.2 g/dL. The serum total IgE level was increased to 246 IU/L (reference range 0-114 IU/L), but skin prick tests with 55 common inhalant allergens were negative. Intradermal tests with 0.1 mg/mL PVC elicited a positive reaction, with a wheal size of 13×10 mm and surrounding erythema of dimensions 24×23 mm. A prick test using PVC gave a negative response. Patch tests with PVC, zinc oxide, Ni and chromium showed a positive result for only Ni at 48 hr.
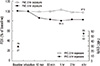
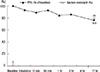
The patient achieved well-controlled asthma with an inhaled corticosteroid and a long-acting beta agonist and was then hospitalized for a specific inhalation challenge test. The methacholine challenge test was positive, with a PC20 value of 2.5 mg/mL. A bronchial challenge test with saline was negative. On the second day, a specific bronchial challenge test in which the patient transferred PVC dust (about 200 mL) between two trays for 2 hr was performed. He complained of coughing and mild itching on his hands, but no significant change in lung function was detected, even the fractional concentration of exhaled nitric oxide (FeNO) was increased. On the third day, a 3-hr bronchoprovocation test with PVC dust was performed using the same procedure. The FEV1 value started to fall about 10 min after exposure and reached a maximum decrease of 19.5% from baseline at 1 hr after exposure (Fig. 1). Several wheals developed on the patient's extremities and abdomen and resolved spontaneously on the day after the exposure. An approximate twofold increase in FeNO (from 29 ppb at baseline to 55 ppb 4 hr after challenge) occurred after a bronchial provocation test with PVC. However, the patient did not expectorate sputum at that time. On the fifth day, a bronchial provocation test with Ni was performed by nebulizing 10-3, 10-2, 10-1, 1, and 10 mg/mL Ni sulfate. A maximum reduction in FEV1 (23.2%) was noted about 17 hr after exposure (Fig. 2). The sputum eosinophil count increased from 2% at baseline to 79% 15 hr after the provocation test.
Based on these findings, the patient was diagnosed with OA caused by both PVC and Ni. After the patient terminated his employment, he had no asthma symptoms and achieved normal pulmonary function through continued inhaled corticosteroid treatment.
DISCUSSION
We diagnosed OA due to exposure to PVC dust and Ni in a patient who had been employed in mixing PVC dust and pulverizing stone at a wallpaper manufacturing factory for several months. Specific inhalation challenge tests with PVC and Ni elicited early and late asthmatic responses, respectively. Furthermore, PVC and Ni skin-test results (positive intradermal test with PVC and a positive response in the Ni patch test) corresponded to the inhalation challenge test results.
The North American Contact Dermatitis Group classified several occupational contact allergens, such as Ni, epoxy resin, formaldehyde, cobalt and chromium, as having established associations with OA (8). The patient had been employed in the roller processing department and subsequently moved to the wallpaper factory, where he handled stone powder. Therefore, he may have been exposed to Ni occupationally, resulting in positive responses to both the patch and bronchial challenge tests with Ni. Moreover, the patient showed a late response to a specific bronchoprovocation test with Ni, a previously identified mechanism of Ni-induced OA (9). In some previous cases, however, specific IgE antibodies to Ni salts conjugated to human serum albumin were detected and showed an early asthmatic response in a specific inhalation test (9, 10).
The pathogenic mechanism of PVC-induced OA has not yet been established. OA associated with PVC exposure is classified as two types. The first is caused by thermoactivated degradation products of PVC and has been reported in meat wrappers exposed to fumes while cutting PVC meat-wrap film using a hot wire. Most of these cases showed respiratory symptoms within 30 min of exposure, but one exhibited a delayed response (7). The second type of PVC-associated OA, of which the present case is an example, is caused by unheated PVC resin dust. While a significant decrease in PEFR was observed beginning 9 hr after bronchial challenge in a previous report (6), the FEV1 in the present case began to decrease 10 min post-exposure, reaching a maximal decrease 1 hr after exposure. Because other laboratory tests, such as skin tests with PVC and sputum analysis, were not performed in the previous case, the pathogenic mechanism of unheated PVC dust was not determined. An early decrease in FEV1 accompanied by a positive intradermal test and an increase in FeNO suggests an allergic sensitization in this case.
The present case suggests that workers can be concurrently exposed to several agents of OA in the same workplace. Cross-reactivity to common proteins or metallic salts was regarded as the mechanism underlying sensitization to multiple agents in the food production or heavy metal industries (11, 12). However, in our case, because no cross-reactivity between PVC and Ni was suspected, two forms of OA associated with different agents may have developed either simultaneously or sequentially.
To avoid further exposure of patients with OA to sensitizers, identification of the causative agents in the working environment is necessary. Besides PVC dust and Ni, phthalates and other metals including chromium, zinc, and copper were suspected as possible causes for the current case. Although it is the best to measure environmental concentration of suspected causes in the workplace, we couldn't monitor working environment at that time. However, because other metals except Ni showed negative responses on the patch test and the patient didn't handle pyrolysis products of phthalates which were certain causes of phthalates-induced OA, we didn't perform provocation test with phthalates and other metals. Although specific inhalation tests using every potential agent remain the standard method for confirmation of the diagnosis of OA, they are currently limited to specialized institutions and there is no standardized protocol. Other methods, including immunologic tests, induced sputum analysis and non-specific bronchoprovocation tests, play a supportive role in a proper diagnosis (13). In addition, the reliability of FeNO measurement in the interpretation of specific bronchial challenge tests with allergens was reported recently. A 12% increase in post-challenge FeNO compared to the baseline value had a high sensitivity and specificity for predicting a positive response in the specific inhalation test (14). The 90% increase in FeNO level 4 hr post-exposure in our case supports the diagnosis of PVC-induced OA.
In conclusion, this case of OA associated with exposure to both PVC dust and Ni emphasizes the need for careful evaluation of agents such as PVC. In spite of whose widespread use, their role in the incidence of OA has been underestimated. Considering also that multiple agents are able to cause occupational sensitization in the same patient, the patient's medical history should be evaluated thoroughly, and specific inhalation tests are essential for diagnosis.
 XML Download
XML Download