

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since the introduction of catheter-based endomyocardial biopsy (EMB) by Sakakibara and Konno in 1962 (1), EMB has been a valuable tool for evaluation of cardiac tissue for cardiomyopathy, myocarditis, unexplained arrhythmia, cardiac tumor, and cardiac involvement of systemic disease. Although the complication rate is not high, this procedure is associated with potentially serious complications. It stands to reason that lowering the incidence of critical complications is a major concern in performing EMB. Fluoroscopic guidance has been used most commonly in this procedure. However, some previous studies have demonstrated the potential benefits of echocardiographic guidance (2-5). The aim of this study was to analyze the complications of transfemoral EMB with single-plane fluoroscopic and two-dimensional (2-D) echocardiographic guidance.
MATERIALS AND METHODS
Patient Selection
A total of 228 consecutive patients who underwent the EMB procedure at Kyungpook National University Hospital from January 2002 to June 2012 were enrolled in this retrospective study. All EMB procedures during this period were performed via the transfemoral approach because of the concurrent diagnostic procedures, such as coronary angiography (CAG). None of them underwent repeated biopsy procedure and all patients were in a nontransplant setting. Data on the patients were collected from medical charts, cardiac intervention reporting database, and echocardiographic and interventional images. A 12-lead ECG was performed before and after the EMB procedure. All patients underwent preprocedural 2-D echocardiography. CAG was performed in 223 patients (97.8%) in order to exclude coronary artery disease as a cause of left ventricular dysfunction and arrhythmia. The results of initial 90 patients were published previously (3).
Echocardiography
Standard 2-D transthoracic echocardiography was performed with System Five (GE Vingmed Ultrasound, Horten, Norway) and Vivid 7 (GE Vingmed Ultrasound, Horten, Norway) before EMB procedures. Left ventricular ejection fraction (LVEF) was determined from apical views using the Simpson biplane formula (6). Interventricular septum (IVS) thickness and left ventricular end-diastolic dimension (LVEDD) were measured in parasternal long axis view. One of three echocardiographic machines were used during the EMB, System Five (GE Vingmed), Vivid-Q (GE Medical Systems, Israel Ltd., Tirat Carmel, Israel) and CX50 (Phillips Ultrasound, Andover, MA, USA).
Endomyocardial biopsy
All EMB procedures were performed by two experienced operators. A 5.5 Fr bioptome (Cordis Corp., Miami, FL, USA) with a length of 104 cm, was used and an 8 Fr Mullins transseptal sheath (Medtronic Inc., Minneapolis, MN, USA) was used for the guidance of bioptome. EMB was performed via the right femoral approach under local anesthesia. After right femoral vein was cannulated, a transseptal sheath was inserted. The sheath tip was placed toward the IVS of the right ventricle (RV) under fluoroscopic guidance and a bioptome was advanced through the sheath. To avoid capturing and damaging tricuspid valve or its subvalvular structure, the jaws of the bioptome remained closed until it touches around apical IVS. Transthoracic 2-D echocardiography was performed by assistant physicians in the opposite side of the operator in order that the operator could also check the echocardiographic images. The tip of bioptome was carefully traced by echocardiography to verify the contact with the IVS. The bioptome was then slowly withdrawn from the apical IVS to mid-IVS, then the jaws of the forcep were opened, and slightly pushed to make firm contact with the IVS. Gentle forward pressure was maintained while the jaws were closed. The specimen was obtained with gentle traction of the shaft of bioptome. Two-D transthoracic echocardiography was repeated immediately after the biopsy procedure and before discharge to check the complications.
Complications
A major complication was defined as procedure-related death or cardiac surgery, pericardial effusion requiring pericardiocentesis, sustained ventricular tachycardia (VT), persistent complete atrioventricular (AV) block, severe tricuspid regurgitation (TR), hemothorax or pneumothorax. Pericardial effusion with no further intervention/treatment, right bundle branch block (RBBB), mild to moderate TR and nonsustained VT were defined as minor complications.
Statistical analysis
Continuous variables were expressed as mean±SD. Comparisons between continuous variables were done by use of Student t-test. Categorical variables were expressed as the number. The chi-square test was used for comparison of categorical variables. A two-tailed P<0.05 was considered statistically significant. Statistical analyses were performed using SPSS® version 20.0 for Windows® (SPSS Inc., Chicago, IL, USA).
RESULTS
Patient characteristics
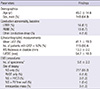
A total of 228 consecutive patients (46.0±14.6 yr-old, 148 male) was analyzed. The study population consisted of 18 patients (7.9%) with assumed myocarditis, 7 patients (3.1%) with suspected infiltrative cardiac disease, 100 patients (43.9%) with unexplained left ventricular dysfunction, 100 patients (43.9%) with unexplained arrhythmia and 3 patients (1.3%) with cardiac tumor. As the study cohort included a large number of patients with cardiomyopathy, echocardiographic data showed a mean LVEF of 41.1%±19.3% and 115 patients (50.4%) had LVEF lower than 50% (Table 1). Among 223 patients who underwent CAG, 209 patients had no significant coronary artery stenosis. In other 14 patients, CAG showed mild (<50%) coronary artery stenosis, which could not explain the clinical condition of the patients. Five patients (2.2%) did not undergo CAG in current study. In two cases of intracardiac mass, there was no need to exclude coronary artery disease. In the other three cases, we could not perform CAG due to acute renal failure or unstable condition of the patients.
During the hospitalization, four patients (1.8%) died. The causes of death were congestive heart failure due to fulminant myocarditis in two cases. One myocarditis patient died of renal failure and another patient with lymphoma expired due to infection after chemotherapy.
EMB procedure
In 217 patients (95.2%), the biopsy specimens were taken only from the IVS of RV. In the other 11 patients (4.8%), in order to enhance the sensitivity, the specimens were taken from specific sites other than IVS, such as RV outflow tract, RV free wall and intracardiac mass. The number of myocardial samples taken by each procedure was 1 to 13 (mean 5.6±2.3) (Table 1).
Complications of EMB
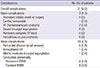
A total of 21 patients (9.2%) experienced complications. There was no case of multiple complications in one patient (Table 2). No case of EMB-related death or surgery was observed in this study.
Major complication; Cardiac tamponade
Cardiac tamponade occurred in one case (0.4%). In this patient, preprocedural echocardiography showed dilated cardiac chambers and decreased wall motion with LVEF of 24%. Ten pieces of specimen were obtained and chest discomfort developed immediately after EMB. Increasing pericardial effusion was observed on 2-D echocardiography and systolic blood pressure was decreased to 60 mmHg. Immediate pericardiocentesis was performed via a subxiphoidal approach and vital signs were stabilized. A total of 300 mL of blood was drained. No further drainage was observed after 24 hr and the catheter was removed. The pathologic diagnosis of this patient was dilated cardiomyopathy (DCMP).
Major complication; Ventricular tachycardia
There were two cases (0.9%) of hemodynamically unstable VT. In both cases, hemodynamically unstable VTs developed during the EMB procedure. Immediate direct current cardioversion restored sinus rhythm and patients were fully recovered without any sequelae in both cases. Final diagnoses of those patients were idiopathic VT and DCMP, respectively.
Minor complication; Pericardial effusion
There were four cases (1.8%) of small pericardial effusion. Two patients had impaired left ventricular systolic function, and the other two patients had normal LVEF. All patients were hemodynamically stable. One of them had mild chest discomfort after the biopsy, however the amount of pericardial effusion was stationary in follow-up echocardiography and the symptom subsided within one day. In all cases, pericardial effusion resolved within a few weeks.
Minor complication; Nonsustained ventricular tachycardia
One case (0.4%) of nonsustained VT was observed. VT with less than 10 ventricular complexes was developed during EMB procedure and the patient had no symptoms. The patient was pathologically diagnosed as DCMP.
Minor complication; Tricuspid regurgitation
New onset TR occurred in one case (0.4%). Clinical diagnosis of the patient was myocarditis. Eight pieces of specimen were obtained during the procedure. Although the patient was completely asymptomatic, follow-up 2-D echocardiography after EMB showed de novo onset of moderate TR, which showed no change during three-years follow-up.
Minor complication; Conduction abnormality
Any degree of AV block was not newly developed after EMB. A total of 12 patients (5.3%) experienced RBBB after the EMB procedure. No underlying left bundle branch block (LBBB) was documented before EMB in those 12 patients. Four cases were permanent and another eight cases were transient. Six patients with transient RBBB recovered within 24 hr after the EMB procedure. In another two patients with transient RBBB, RBBB resolved within one and three months after EMB, respectively.
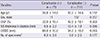
Analysis of the incidence of complications according to the etiology of heart disease showed a trend of higher complication rate in the cardiomyopathy group (Fig. 1). Among the thirteen cases of complications developed in cardiomyopathy group, nine cases were RBBBs. It seemed that RRRBs drove such a tendency of high complication rate in cardiomyopathy group. LVEF was significantly lower and left ventricular dilatation was more severe in patients with EMB related complications than in those without. However, there were no significant differences in age, gender, IVS thickness, and number of biopsy specimen between the two groups (Table 3). There was no significant inter-operator difference in overall complication rate (7.0% vs 10.9%, P=0.308).
DISCUSSION
EMB has an important role in the diagnosis of unexplained cardiomyopathies (7), unexplained arrhythmias (8-10), cardiac infiltrative diseases (11-13), and cardiac tumors (14,15). Furthermore, in patients with myocarditis, EMB provides not only diagnostic clues but also therapeutic and prognostic implications (16, 17). Despite all advantages of EMB-based diagnosis, EMB procedure itself is perceived to carry a high risk of major adverse events, such as cardiac tamponade and some raise a question about the role of EMB in the era of new cardiac imaging modalities such as cardiac magnetic resonance imaging (18, 19). However, histological confirmation is still needed in many patients in whom non-invasive evaluation is inconclusive. Our analysis of 228 consecutive EMB procedures with fluoroscopic and 2-D echocardiographic guidance showed very low complication rate, especially with major complications. Major complication rate of this study was 1.3% (n=3), with one case (0.4%) of cardiac tamponade and two cases (0.9%) of sustained VT. Neither procedure related mortality nor surgery was developed. Although four cases of in-hospital death was observed in this study, no direct association was observed between the cause of their deaths and EMB.
Cardiac tamponade is one of the most concerned complications for physicians performing EMB. In the earlier surveys of fluoroscopy-guided RV EMB procedures, Yilmaz et al. reported the higher incidence of cardiac tamponade as 0.8% (n=4 of 490) than our data (20). Deckers et al. (21) reported the similar incidence of cardiac tamponade as 0.4% (n=2 of 546) to our data (n=1 of 228); however, the two cases in their study were related to mortality after all. Both 2-D echocardiography and fluoroscopy were utilized as a guiding method for biopsy in our study and our data seemed to show less critical complications compared to earlier two studies. Use of 2-D echocardiography in addition to fluoroscopic guidance allows better visualization of the soft tissue structure of the heart and the tip of the bioptome. Identification of the contact between the tip of the bioptome and myocardium could decrease the risk of cardiac perforation. Echocardiography can also provide a sensitive and reliable detection of new or increasing pericardial effusion when cardiac perforation occurs and appropriate management can be applied without delay. In practice, prompt detection of emerging pericardial effusion by echocardiography could enable immediate pericardiocentesis and stabilization of the patient with cardiac tamponade in our study cohort. Another advantage of using echocardiographic guidance for EMB is that myocardial sampling from specific location is possible in the case of heterogeneous myocardial pathology, such as cardiac tumors or suspected focal myocarditis. In addition, echocardiographic guidance can reduce radiation exposure. The operator can easily confirm the direction of the bioptome toward the target site, such as IVS, RV outflow tract, and RV free wall, by 2-D echocardiographic guidance and it can possibly reduce fluoroscopy time.
TR occurs frequently among cardiac transplantation recipients because of repeated biopsies. Previous studies reported rates of severe TR up to 6.8% in posttransplant EMB procedures (22-25). However, the incidence of TR among nontransplant patients is not well known. In current study with nontransplant patients, incidence of tricuspid valve injury was low (n=1 of 228, 0.4%). Although, 2-D echocardiography has limitations in that the current resolution is not sufficient for direct visualization of chordae tendineae, 2-D echocardiographic guidance might reduce the occurrence of valve injury by visualizing both the tip of bioptome and cardiac tissue around the tip of bioptome. Recent advances in echocardiography, including real-time 3-D echocardiography, may allow for better visualization of heart structure and biopsy instruments (26, 27).
In terms of conduction disturbance, Deckers et al. (21) reported 0.2% (n=1 of 546) of RBBB and 0.6% (n=3 of 546) of complete AV block and Yilmaz et al. (20) reported 0.2% (n=1 of 490) of complete AV block requiring insertion of temporary pacemaker. In our study, all 12 conduction disturbances (5.3%) were presented as RBBBs and no transient or permanent AV block was observed. In 14 patients with preexisting LBBB before EMB, no RBBBs were developed after the procedure in our study. However, there is a high risk of AV blocks causing hemodynamic instability in patients with preexisting LBBB and proper preparation of temporary pacemaker must be needed in the procedure of such patients. Compared to two previous studies, we could not reduce the incidence of RBBB despite the dual guidance of 2-D echocardiography and fluoroscopy. There seem two possibilities. The first one is that, as the bundle branch is invisible structure by echocardiography or fluoroscopy, damage to the bundle branch cannot be prevented. The other is that echocardiographic guidance guides the tip of forcep to some specific area of IVS around right bundle branch, resulting in higher chance of damage on right bundle branch.
In our study, cardiomyopathy group showed a trend of higher overall complication rate, in which the incidence of RBBB seemed to be a major contributor. Our data also showed that decreased LVEF and left ventricular dilatation were associated with the occurrence of complications. One possible explanation is that conduction system, with the pathologic process of cardiomyopathy, might be more easily damaged. The studies of Akar et al. and Glukhov et al. reported that there is a conduction slowing in various cardiomyopathies and the nature of it varies depending on disease etiology (28-30). The conduction system of such pathologic condition might be prone to be damaged by mechanical irritation during the biopsy procedure and that could make a higher risk of developing RBBB. Another possible explanation is that dilated chambers in cardiomyopathies can make more obtuse angle between the inferior vena cava and the longitudinal axis of the tricuspid valve and bioptome should approach the IVS with more obtuse angle. Such alteration may guide the tip of bioptome to more specific site, which can damage to right bundle branch more easily.
In conclusion, transfemoral EMB with fluoroscopic and 2-D echocardiographic guidance is a safe procedure with low complication rate. Left ventricular dysfunction and increased left ventricular dimension may be related to the occurrence of complications in EMB.

 XML Download
XML Download