

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Recurrent ischemic events after acute coronary syndrome (ACS) still remain common. Anti-thrombotic therapy with coronary revascularization and high rates of procedural success reduce the frequency of life-threatening ischemic events (1-3). However, with the greater use of anti-thrombotic medications and early revascularization, bleeding has become an increasingly important problem. Recently, the European Society of Cardiology guidelines are recommended to evaluate bleeding risk in non-ST elevation (NSTE)-ACS patients using established risk scores for bleeding such as the Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA guidelines (CRUSADE) bleeding risk score (4, 5). This score is relatively accurate for estimating bleeding risk by combining patient's clinical variables. It is well known that bleeding complication is a strong independent predictor of early and late adverse clinical outcome in NSTE-ACS patients. Therefore, all efforts should be made to reduce bleeding whenever possible, especially in patients with high risk of bleeding. However, whether vascular access affect in-hospital major bleeding (IHMB) in patients with ACS, especially at high-bleeding risk, is not well determined. Therefore, the aim of our study is to evaluate the association between vascular access and IHMB in ACS patients with moderate- to very high-CRUSADE bleeding risk.
MATERIALS AND METHODS
Study population
The trans-radial intervention (TRI) registry is a retrospective, observational, on-line registry data of all-comers who received the percutaneous coronary intervention (PCI) in 16 institutes of Korea from January through December 2009. The aim of registry is to evaluate the safety and efficacy of TRI compared with the trans-femoral intervention (TFI) in Korean patients. The vascular access for patient (trans-radial or trans-femoral) was determined by the clinical decision of interventional cardiologist in each institutes. The data including baseline clinical, laboratory, angiographic characteristics, and 1-yr clinical outcomes were collected by a specialized study coordinator at each center using a standardized case report form. TRI or TFI was classified according to final vascular access without regard to operators' intention before the index procedure.
Total 4,072 patients were enrolled in TRI registry and 2,027 patients were diagnosed with non-ST elevation myocardial infarction (NSTEMI) or unstable angina. The difference between NSTEMI and unstable angina was whether the cardiac markers were elevated or not. Of them, 995 patients with the CRUSADE moderate- to very high-bleeding risk scores (bleeding scores more than 31) were selected. Among them, 402 patients received coronary intervention via trans-radial approach (TRI group) and 593 patients via trans-femoral approach (TFI group) (Fig. 1).
Procedure and post-intervention medications
The emergent or early invasive treatments were determined based on the ACS patient status according to the clinical decision of operators in each institutes. The type of stent and use of peri-procedural glycoprotein IIb/IIIa inhibitors and anti-thrombotic medications were also determined based on the decision of operators and current guidelines. Percutaneous closure devices were unrestrictedly used to close arterial punctures. Anti-platelet agents were administered to all patients prior to the intervention, with aspirin 300 mg and clopidogrel 300-600 mg. After the intervention, the patients received 100 mg of aspirin per day indefinitely and 75 mg of clopidogrel per day for at least one year. Other medical treatments were also used based on the standard treatment regimen for patients with ACS in a non-restrictive manner.
CRUSADE bleeding scores
For each patient, the CRUSADE risk score was calculated from the corresponding scores for the 8 prognostic variables it involves. The CRUSADE bleeding score considers baseline patient characteristics (female sex, history of diabetes, prior vascular disease), admission clinical variables (heart rate, systolic blood pressure, signs of congestive heart failure), and admission laboratory values (hematocrit, calculated creatinine clearance) (5).
Study outcomes
The primary end-point was the incidence of IHMB as defined in the CRUSADE study, such as intracranial bleeding, documented retroperitoneal bleeding, a fall in hematocrit of ≥12% (baseline to nadir), or any red blood cell transfusion in which baseline hematocrit was ≥28% or <28% with clinically documented bleeding. In patients who underwent revascularization surgery, only major bleeding events that occurred before the intervention were taken into account. Renal clearance of creatinine was calculated with the Cockcroft-Gaut formula. The definition of prior vascular disease was also that adopted by the CRUSADE registry (prior stroke and/or peripheral artery disease). The secondary end-point was the incidence of the 1-yr major adverse cerebro-cardiovascular events (MACCE) defined as the composite of all-cause mortality, non-fatal MI, target lesion revascularization (TLR), stent thrombosis, and cerebro-vascular accidents (CVA). TLR was defined as any ischemic driven percutaneous coronary revascularization performed on the treated lesion or vessel. Stent thrombosis was defined according to the Academic Research Consortium of Circulatory System Devices Panel Meeting, an advisory committee to the US Food and Drug Administration (FDA) in 2006.
Statistical analysis
Continuous variables were expressed as mean ± SD and categorical ones were expressed as a frequency. An analysis of continuous variables was performed using Student's t-test and that of categorical ones was performed using chi-square test or Fisher's exact test. Multiple logistic regression analysis with the forward LR (likelihood ratio) was used to identify the independent predictors of IHMB. Only variables with a P value < 0.2 in the univariate analysis were included in the multivariate model. All the statistical analyses were performed using SPSS 18.0 (Statistical Package for Social Science, SPSS Inc, Chicago, IL, USA) for Windows. All statistical tests were two-tailed, and a value of P < 0.05 was considered statistically significant.
RESULTS
Patient baseline characteristics
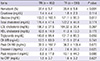
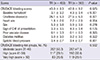
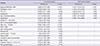
Baseline demographic and clinical characteristics and laboratory findings of the 2 groups are shown in Table 1 and Table 2. Current smoker, the past history of MI and heart failure were more common in TRI group. However, the past history of bypass surgery and stable hemodynamic conditions at admission were more common and baseline hematocrit and creatinine clearance were lower in TFI group. The CRUSADE bleeding scores and risk groups were no significantly different between two groups (Table 3). Six hundred mg loading dose of clopidogrel and use of low molecular weight heparin were more common in TRI group, however, use of unfractionated heparin or glycoprotein IIb/IIIa and ACC/AHA B2/C lesions were more common in TFI group. Six-French arterial sheath was commonly used in TRI group, but seven-French sheath in TFI group. Total numbers of treated lesions were higher and procedure times and fluoroscopy times were significantly longer in TRI group, however, the vascular access site complications were similar between two groups (Table 4).
Clinical outcomes
During 1-yr clinical follow-up, the incidence of in-hospital mortality and 1-yr MACCE were no significantly different between two groups (4.2% vs 3.9%, P = 0.783; 11.2% vs 14.8%, P = 0.097). However, the incidence of IHMB and blood transfusion were significantly lower in the TRI group compared with TFI group (6.0% vs 9.4%, P = 0.048; 4.5% vs 9.4%, P = 0.003) (Table 5). The incidence of IHMB showed a consistent gradient of risk across the 3 risk categories, regardless of vascular access. The incidence of IHMB was no significantly different between two groups in patients with the CRUSADE moderate bleeding risk (3.0% vs 2.8%, P = 0.931). However, TRI group tended to have lower incidence of IHMB than TFI group in patients with the CRUSADE high- and very high bleeding risk group (4.3% vs 9.9%, P = 0.073; 15.7% vs 24.4%, P = 0.134) (Fig. 2). Accordingly, the significant lower incidence of IHMB in patients with CRUSADE high to very high bleeding risk group (n = 511) was observed in TRI group than TFI group (9.0% vs 15.4%, P = 0.034). The eighty patients (8.0%) suffered from IHMB. Retroperitoneal bleeding occurred in two patients of TFI group, hemoptysis in one patient of TFI group, and gastrointestinal bleeding in three patients of each group. They had higher incidences of in-hospital and 1-yr mortality than those free from IHMB (3.1% vs 15.0%; 7.2% vs 30.0%, P < 0.001 respectively) (Fig. 3, 4).
Multivariate and subgroup analyses
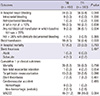
By multivariate logistic regression analysis, the independent predictors of IHMB were the diagnosis of NSTEMI (odds ratio [OR], 3.152; 95% confidence intervals [CI], 1.720-5.775), hematocrit <31% at admission (OR, 2.715; 95% CI, 1.476-4.994), the use of glycoprotein IIb/IIIa inhibitors (OR, 3.226; 95% CI, 1.257-8.281), and the history of hypertension (OR, 2.490; 95% CI, 1.106-5.608). However, TRI group (OR, 0.359; 95% CI, 0.181-0.712), the history of dyslipidemia (OR, 0.364; 95% CI, 0.177-0.748) were the independent negative predictors of IHMB (Table 6).
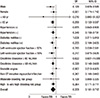
Subgroup analyses showed that compared to TFI, TRI could significantly reduce the incidence of IHMB in male gender (OR, 0.129; 95% CI, 0.029-0.586; P = 0.008), in patients older than 65 yr (OR, 0.280; 95% CI, 0.133-0.587; P = 0.001), in patients with the history of hypertension (OR, 0.340; 95% CI, 0.158-0.731; P = 0.006), in patients with the history of diabetes (OR, 0.255; 95% CI, 0.104-0.626; P = 0.003), in patients with creatinine clearance less than 60 mL/min (OR, 0.320; 95% CI, 0.149-0.689; P = 0.004), in patients with left ventricular ejection fraction less than 50% (OR, 0.217; 95% CI, 0.075-0.626; P = 0.005), in patients with NSTEMI (OR, 0.267; 95% CI, 0.108-0.660; P = 0.004), and in patients with the high- to very high-bleeding risk (OR, 0.364; 95% CI, 0.171-0.777; P = 0.009) (Fig. 5).
DISCUSSION
Our study was conducted to determine the impact of vascular access on IHMB and mortality in NSTE-ACS patients with moderate- to very high-bleeding risk. Although numerous studies have reported the association between vascular access and IHMB, previous studies did not focus precisely patients with high bleeding risk. Our study showed that regardless of vascular access, the incidence of bleeding was also higher among the CRUSADE highest risk groups in Korean patients and IHMB was still significantly correlated with in-hospital and 1-yr mortality. Our study suggests that compared to TFI, TRI could reduce IHMB on ACS patients with the CRUSADE moderate- to very high-bleeding scores.
Patients with ACS are typically managed by initial medical stabilization followed by an early invasive approach, whereby cardiac catheterization is performed, usually within 24-48 hr of admission and the majority of patients subsequently undergo PCI. Use of anticoagulant and antiplatelet agents with early, invasive management reduces the risk for recurrent ischemic events, but may increase the risk for bleeding (6).
The incidence of bleeding complications varied widely among different trials. These discrepancies are primarily due to the different definitions of major bleeding used and the different or new anti-thrombotic agent regimens used in the each trial. From analysis of 302,152 patients who performed PCI procedure at the 440 United States centers, bleeding complications occurred in 2.4% of patients (7). In the OASIS-5 study, the rate of MB at nine days was markedly lower with fondaparinux than with enoxaparin (2.2% vs 4.1%; hazard ratio, 0.52; P < 0.001) (8). In addition, a non-CABG-related MB occurred within 30 days of randomization in 520 (3.8%) of the 13,819 ACUITY patients and in 224 (6.2%) of the 3,602 HORIZONS-AMI patients (9, 10). The rate of bleeding complication seemed to be more prevalent in patients with ACS or AMI than those with stable angina. Our study represented that the rate of IHMB was 8.0%. The rate of bleeding was likely to be similar or somewhat higher compared with those of the other studies. It is explained that our study was not a well-controlled randomized trial but a real-world clinical practice and enrolled the NSTEMI or unstable angina patients with moderate to very high bleeding risk. The incidence of MB also showed a consistent gradient of risk across the 3 risk categories in our study. Regardless of vascular access, bleeding incidence was higher among the CRUSADE highest risk groups. The CRUSADE bleeding risk score groups were also well correlated with the incidence of IHMB in Korean NSTE-ACS patients.
It has been well known that MB was strongly associated with increased mortality. In addition, the severity of the bleeding complications was directly correlated with worse outcomes (11-14). A recent study from the CRUSADE registry reported that IHMB was a significant association with short and long-term mortality, particularly among PCI-treated patients with NSTEMI (15). In long-term data from HORIZON-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction), the patients with IHMB after primary PCI have significantly increased 3-yr rates of morbidity and mortality (16). Many mechanisms that MB affects worse outcomes might involve greater comorbidities (advanced age, impaired glomerular filtration rate, diabetes, etc.) in bleeding patients, anemia results in an impairment of the oxygen delivery, hypotension, transfusion, inflammatory response and early cessation of antithrombotic therapies because of bleeding (17-19). Our study showed that IHMB was also significantly associated with in-hospital and 1-yr mortality.
A large number of trials have reported the predictors of MB including advanced age, female gender, baseline anemia, impaired renal function, previous history of bleeding, STEMI, advanced Killip class (III or IV) the degree of excess dose and the number of antithrombotic agents such as heparin plus glycoprotein IIb/IIIa inhibitor (17, 18, 20-24). In our study, initial diagnosed as NSTEMI, hematocrit <31%, use of glycoprotein IIb/IIIa inhibitor, and history of hypertension were also significant predictors of IHMB, however, TRI was a negative predictor. Probably, it was associated that trans-radial access could reduce the access site-related bleeding complications.
Bleeding complications after PCI are most commonly related to vascular access site and are associated with an increased risk of post-PCI morbidity and mortality (25-27). Pooled analysis of 23 randomized trials (n = 7,020) comparing the association between radial versus femoral approaches for PCI presented that radial access reduced major bleeding and there was a tendency for reduction in ischemic events compared to femoral access (28). A recent study presents that TRI is associated with decreased 2-yr mortality rates and a reduction in the need for vascular surgery and/or blood transfusion compared with TFI in patients undergoing angioplasty for AMI (29). Our study showed that TRI was also significantly related with reduction of IHMB and blood transfusion, however, resulted in similar rates of in-hospital mortality and 1-yr MACCE compared with TFI. Probably, our study showed relatively low incidences of major bleeding related to vascular access, and in addition, more than half of IHMB in TFI were any red blood cell transfusion in which baseline Hct ≥28%, which could be possible a clinically insignificant state. Therefore, vascular access could have less influence on the mortality in our study. However, it was still uncertain that TRI could reduce short- and long-term mortality and large trials were necessary to discuss about this issue.
Our study showed that TRI was associated with a significant reduction in IHMB that was more prominent in patients with high-risk subgroups, such as more than 65 yr, history of hypertension and diabetes, low left ventricular ejection fraction, impaired renal function, NSTEMI and high- to very high-bleeding risk. Therefore, TRI was more safe and efficacious than TFI in patients with ischemic risk as well as those with bleeding risk.
Our study has some limitations. First, our study was a multi-center retrospective observational registry study that was many missing values. Therefore, the CRUSADE bleeding risk scores were relatively underestimated and the portion of moderate- to very high-bleeding risk group in our registry was relatively smaller than that in real-world clinical practice. We thought that our study was underpowered to assess the 1-yr clinical outcome. However, in our study, it is clear that TRI had lower incidences of blood transfusion and IHMB than TFI in ACS patient with moderate- to very high bleeding risk. Second, our study was a retrospective post-hoc subgroup analysis of a TRI registry where the selection of vascular access was determined by the attending interventional cardiologists and we did not apply the propensity score matching analysis for elimination of the observed differences. Therefore, this might have introduced a significant bias in patient selection, even though it was partially compensated by multivariate analysis to control the baseline biases. Third, in spite of no interaction between vascular access and use of glycoprotein IIb/IIIa inhibitors in logistic regression analysis, TRI group was less frequent use of glycoprotein IIb/IIIa inhibitors than TFI group.
In conclusions, our study represents that IHMB is still significantly correlated with in-hospital and 1-yr mortality and the CRUSADE bleeding risk score groups are also well correlated with the incidence of IHMB in Korean NSTE-ACS patients. Furthermore, we conclude that compared to TFI, TRI could reduce IHMB in ACS patients with the CRUSADE moderate- to very high-bleeding scores. However, much more trial remains to be done on the beneficial effect of TRI for clinical outcomes.






 XML Download
XML Download