

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Colorectal cancer (CRC) is the second-leading cause of cancer-related deaths (1), and approximately 143,460 new cases are diagnosed each year in the United States (2). In Korea, incidence rates of CRC have also markedly risen over the past few year (3). Most human CRC begins as a benign adenomatous polyp, which develops into an advanced adenoma with high-grade dysplasia and then progresses to invasive cancer (4). Strategies for preventing CRC often focus on preventing the development of colonic adenomas that are the precursors of invasive CRCs (1). Hence, there is an increasing demand for biomarkers that can assess risk and provide the early detection of colonic adenomas (5).
The activation of prostaglandin signaling is an early and critical step in the development of colon adenomas (1, 4, 6). Cyclooxygenase-2 (COX-2) catalyzes prostaglandin E2 (PGE2) synthesis, which is a well-known early oncogenic event in colonic carcinogenesis (7). PGE2 levels are also regulated by degradation, and 15-hydroxyprostaglandin dehydrogenase (15-PGDH) is the first rate-limiting enzyme for the inactivation and degradation of PGE2 (8). Previously, it was reported that 15-PGDH is not expressed in CRC (9, 10), and that 15-PGDH is downregulated during the early stages of colonic tumorigenesis (9). Recent studies have reported that β-catenin represses 15-PGDH expression in colon tumorigenesis, possibly even before the upregulation of COX-2 (11). Therefore, the suppression of 15-PGDH in the colorectal mucosa can lead to sporadic colorectal neoplasias and is involved in the early stages of colorectal tumorigenesis, prior to changes in COX-2 expression.
Human CRC usually develops in mucosa that has already undergone multiple genetic changes. These changes create "field effect" that are characterized by the presence of morphologically normal but biologically altered epithelial cells (12). The presence of a field with genetically altered cells is a risk factor for cancer. Therefore, the detection and monitoring of the field may have profound implications in cancer prevention.
Clinical studies on the use of single genetic markers to predict field effect in colorectal carcinogenesis are lacking because multiple genetic changes are involved in the field effect in colorectal tissue. We hypothesized that 15-PGDH could be a potential source of field effect in the colorectal mucosa because it is involved in the early stages of colorectal carcinogenesis and regulates prostaglandin, which plays an important role in colorectal carcinogenesis. Furthermore, 15-PGDH in colorectal mucosa could be a useful biomarker for risk assessment and the early detection of colonic adenomas.
The aim of our present study was to investigate the potential role of 15-PGDH in normal-appearing colorectal mucosa as a biomarker for the prediction of synchronous colorectal adenomas and future adenomas.
MATERIALS AND METHODS
Study population
The study population consisted of 32 patients who had undergone curative surgical resection for the treatment of primary sporadic CRC at Asan Medical Center (Seoul, Korea) from 2005-2007. Using the patient database, we retrieved the cases without the following factors: prior history of CRC, inflammatory bowel disease, use of nonsteroidal anti-inflammatory drugs (NSAIDs) in the last six months, history of preoperative chemotherapy or radiotherapy, incomplete examination of the entire colon prior to surgery, and < 2 follow-up colonoscopies. Of these 32 CRC patients, 24 had colon cancer and the remaining 8 had rectal cancer. All 32 patients had a single cancer lesion.
Sample collection and data analysis
We used the surgical specimens stored at the Biological Resource Center at Asan Medical Center. We obtained paired tumor and normal colon tissues from the surgical specimens that were taken from each patient. We used the term "normal-appearing colorectal mucosa" to describe colorectal mucosa that is grossly and pathologically normal but might be genetically altered. We obtained normal-appearing colorectal mucosa from the margins of the CRC surgical specimens. An expert gastrointestinal pathologist confirmed if the specimens contained a tumor or were normal.
In all 32 cases in our study cohort, the first follow-up colonoscopy was performed within 1.5 yr of surgery. The adenoma detected on the first follow-up colonoscopy was considered to be missed lesions of the preoperative colonoscopy; therefore, we defined synchronous adenoma (SA) as adenoma detected on the preoperative colonoscopy and the first follow-up colonoscopy. We classified the CRC patients into two groups according to the presence of SA; SA group or NSA (non-SA) group. The "SA group" included CRC patients with SA and the "NSA group" included CRC patients without SA. We evaluated the association between 15-PGDH mRNA expression and each group. We defined metachronous adenoma (MA) as adenoma that was detected on the second and subsequent follow-up colonoscopy. We evaluated the cumulative incidence of MA and its association with 15-PGDH mRNA expression. The "low-PGDH group" included CRC patients with 15-PGDH mRNA expression in normal-appearing colorectal mucosa that was less than the median value, and the "high-PGDH group" included CRC patients with 15-PGDH mRNA expression that was greater than the median value.
Quantitative real-time PCR assay
We assayed the relative mRNA expression of 15-PGDH in the paired tumor and normal colon mucosa using quantitative real-time PCR. Total RNA was extracted using the RNeasy kit (Qiagen, Germantown, MD, USA). The concentration and quality of the RNA samples were determined using a Nanodrop-1000 spectrophotometer (NanoDrop Technologies, Montchanin, DE, USA). Samples were processed using cDNA with MultiScribe™ Reverse Transcriptase (Applied Biosystems, Foster city, CA, USA), and 40 ng of each sample was used in the real-time PCR assays in order to determine 15-PGDH expression. Real-time PCR was performed using the Applied Biosystem 7500 Real-Time PCR system. Real-time PCR of 15-PGDH was performed using the human 15-PGDH TaqMan Probe/Primer kit (Hs 00168359_mL; Applied Biosystems). β-Actin was amplified using the human ACTB TaqMan primer/probe kit (Hs 99999903-mL; Applied Biosystems). Relative gene expression was normalized to the mRNA of β-actin and calculated using the 2-ΔΔCt method.
Statistical analysis
Statistical analyses were performed using Statistical Package for the Social Sciences (version 18.0; SPSS Inc., Chicago, IL, USA). Differences in the continuous variables of the two groups were evaluated using the Student t-test or Mann-Whitney U test. Differences in the paired continuous variables of the two groups were evaluated using the Wilcoxon signed-rank test. Differences in the continuous variables between the three groups were evaluated using the Kruskal-Wallis test. Differences in the categorical variables were evaluated using the chi-square test or Fisher's exact test. Logistic regression models were used to predict SA risk factors in CRC patients. Correlations between the factors were analyzed by calculating the Pearson's correlation coefficients (r and P). The Kaplan-Meier method was used to calculate the cumulative rate of MA, and the log-rank test was used to determine the differences between all groups. Cox proportional-hazards regression modeling was used to estimate the relative risk of MA. All P values < 0.05 were considered statistically significant.
RESULTS
15-PGDH mRNA expression is downregulated in CRC
In total, 32 CRC patients (21 males [65.6%]; median age, 60 yr [range: 45-73 yr]) were analyzed. To confirm the repression of 15-PGDH expression in the cancer tissues, we examined 15-PGDH mRNA levels in paired cancer and normal tissues. As previously reported (9, 10), relative 15-PGDH mRNA expression was downregulated in cancer tissues in comparison with normal tissues (P < 0.001); the relative mean level of 15-PGDH mRNA expression in cancer tissues was significantly lower than that of the matched normal-appearing mucosa (0.07 vs 1.00; P < 0.001; Fig. 1A).
Clinical characteristics of the study population
Of the 32 CRC patients, 13 patients (40.6%) had SA (SA group) and the remaining 19 patients (59.4%) did not have SA (NSA group). The mean number of SAs was 5.54 (range: 1-16), and 9 patients (69.2%) had ≥ 3 SAs. The mean adenoma burden (sum of the largest diameters of the adenoma) of the SA group was 33.69 mm (range, 3-136), and 7 CRC patients (53.8%) were diagnosed with advanced SA.
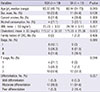
The clinicopathological characteristics of the SA and NSA groups are shown in Table 1. The patients in the SA group were older than the patients in the NSA group (62.44 yr vs 55.37 yr; P = 0.013). However, no significant differences were determined between these two groups in terms of sex, smoking status, alcohol consumption, body mass index, cholesterol level, or family history of CRC. Of the 32 patients in our study cohort, 8 (25.0%), 13 (40.6%), and 11 (34.4%) were categorized with stage I, II, or III tumors, respectively, according to the National Comprehensive Cancer Network (NCCN) TNM staging system. No patients in either group had a metastatic lesion. The two groups did not differ in terms of cancer stage. However, the SA group demonstrated more advanced tumors, in terms of T stage, than the NSA group. In the SA group, 92.3% of patients were classified with T3 stage tumors, whereas 52.6% of the NSA group (P = 0.018) was classified with T3 stage tumors.
15-PGDH in normal-appearing colorectal mucosa is downregulated in CRC patients with SA
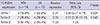
To determine if 15-PGDH is downregulated in normal-appearing colorectal mucosa in patients with SA, we examined the 15-PGDH mRNA levels in this tissue. The relative mean level of 15-PGDH mRNA expression in the SA group (0.71; range: 0.08-2.03) was significantly lower than in the NSA group (1.00; range, 0.26-1.52; P = 0.044; Fig. 1B). Table 2 presents the relative 15-PGDH mRNA expression levels of normal-appearing colorectal mucosa according to the participant characteristics at baseline. 15-PGDH mRNA expression in normal-appearing colorectal mucosa was significantly lower in the SA group compared with the NSA group, as mentioned previously. However, there were no significant differences between any of the other clinicopathological characteristics, including age and T stage.
Table 3 presents the results of the logistic regression modeling of the relationship between 15-PGDH mRNA expression in normal-appearing colorectal mucosa and the presence of SA. CRC patients in the lowest tertile of 15-PGDH mRNA expression in normal-appearing colorectal mucosa were most likely to have SA (odds ratio, 10.5; 95% confidence interval, 0.01-0.74). We also investigated if the characteristics of SA are related to 15-PGDH mRNA expression in normal-appearing mucosa. However, there was no correlation found between 15-PGDH mRNA expression and the mean number of SAs (r = -0.02; P = 0.947) or between 15-PGDH mRNA expression and SA burden (r = 0.02; P = 0.940).
15-PGDH in normal-appearing colorectal mucosa and the risk of new adenomas
We investigated whether 15-PGDH mRNA expression in normal-appearing colorectal mucosa can be used to predict the risk of future adenomas. The median postoperative follow-up period was 52 months (range, 24-63 months), and the average number of surveillance colonoscopies was 4.28 in our current CRC patient series. No cancer recurrence was noted during the follow-up period. Of the 32 CRC patients studied, MAs were detected in 15 cases (46.9%) during the follow-up period.
The clinicopathological characteristics of the low- and high-PGDH groups are shown in Table 4. The low-PGDH group demonstrated more advanced stage cancers than the high-PGDH group; patients with stage III cancer comprised 47.1% of the low-PGDH group and only 20.0% of the high-PGDH group (P = 0.045). Additionally, even though its significance was only borderline, the low-PGDH group demonstrated more advanced T stage tumors than the high-PGDH group; patients with T3 stage cancer comprised 82.4% of the low-PGDH group and only 53.3% of the high-PGDH group (P = 0.089). The low-PGDH group had more patients with SA than the high-PGDH group (58.8% vs 20.0%; P = 0.036). There were no significant differences between these two groups in terms of any of the other clinicopathological characteristics.
To determine if 15-PGDH expression in normal-appearing colorectal mucosa is related to the development of new adenomas, we examined the cumulative incidence of MA according to the baseline 15-PGDH mRNA expression levels of normalappearing colorectal mucosa. The results showed no significant differences in terms of the cumulative incidences of the low- and high-PGDH group (P = 0.333; Fig. 2). Table 5 presents the relative risks of various patient characteristics and SA characteristics for MA. The hazard ratios for MA did not differ significantly, regardless of any of the clinicopathological characteristics.
DISCUSSION
Our present study findings demonstrate that the downregulation of 15-PGDH, a tumor suppressor, can be used as a biomarker of field cancerization. Low 15-PGDH expression in normal-appearing colorectal mucosa is associated with more advanced stage tumors as well as presence of synchronous adenomas in sporadic CRC patients.
The presentation of CRC can be divided into three patterns: sporadic, inherited, and familial. Among these, the sporadic form of the disease, in which there is no family history, accounts for approximately 70% of all CRC cases. Environmental and genetic factors can increase the likelihood of developing sporadic CRC (13). However, the use of clinical factors as predictors have limited value because most clinical risk factors are thought to confer a small or uncertain magnitude of risk, and it is difficult to accurately investigate the combination effects of various factors. Hence, the determination of a novel biomarker that reflects cancer risk is required for the early detection of sporadic colorectal neoplasms.
Human CRC is a typical example of the multistep progression of cancer, and genetic changes have been shown to occur before CRC develops (14). "Field effect" includes the presence of ≥ 1 areas comprising epithelial cells that have been genetically altered, and this area precedes and is predisposed to the development of cancer (15). The concept of "field effect" was first introduced in 1953 to explain the development of multiple primary tumors and locally recurrent cancer (16). In CRC, the field effect is also characterized by the simultaneous development of multiple but distinct tumors, which are either separate malignancies or a single malignancy that is accompanied by multiple preneoplastic lesions (12, 17). Epigenetic defects, such as the methylation of the DNA repair gene O6-methylguanine-DNA methyltransferase (MGMT) in normal colorectal mucosa, have been proposed as potential sources of field effect during colon carcinogenesis (17-19). Apoptosis in the normal rectal mucosa has also been proposed as a predictor of synchronous colon adenoma and the development of future adenomas (20, 21). However, the identification of the genes that identify individuals who are at risk of CRC is lacking. There has only been one previous study on the association between p53 and field effect in colon cancer (22), but the clinical implications of this earlier report are unclear.
Our current findings show that 15-PGDH expression in normal-appearing colorectal mucosa is downregulated in CRC patients with synchronous adenoma, and that CRC patients with relatively low 15-PGDH mRNA expression in normal-appearing colorectal mucosa are the most likely to have SA. These findings suggest the existence of a field effect in the colon that predisposes individuals with lower levels of 15-PGDH to the development of adenomas. Our present findings also show that the SA group demonstrated more advanced T stage tumors than the NSA group and that the low-PGDH group demonstrated more advanced stage cancers than the high-PGDH group. Additionally, although not statistically significant, the higher T stage tumors and higher stage cancers tended to demonstrate lower 15-PGDH expression in normal-appearing mucosa. These findings suggest that the genetic alteration of the surrounding normal-appearing mucosa accelerates tumor growth. Our group has shown that knocking out the murine 15-pgdh gen markedly sensitizes normally resistant C57BL/6J mice to colon tumor induction by carcinogen azoxymethane (9). Tumors can easily occur in the genetically altered mucosal environment; therefore, low 15-PGDH expression of normal-appearing mucosa around the tumors may have contributed to tumor growth. In summary, the results of the present study suggest that 15-PGDH could be a potential source of field effect in colorectal mucosa. Moreover, 15-PGDH could be a potential biomarker for the prediction of colorectal neoplasms.
Contrary to our hypothesis, 15-PGDH in normal colorectal mucosa did not predict the risk of developing new adenomas. One possible explanation for this result is that some other molecular marker or clinical factor that was not measured in this study also has a dominant effect on the development of new adenomas. Possibly due to the small sample size, our data do not indicate any risk factor for the development of new adenomas, even though various risk factors are known (23, 24). Although not statistically significant, the Kaplan-Meier graph showed a tendency for the higher cumulative incidence of MA in the low-PGDH group. Larger prospective studies are needed to confirm these findings.
Our present findings show that the patients in the SA group had a higher mean age than those in the NSA group. Older age also demonstrated a significant effect on the development of adenomas (23), and therefore age might be a confounding factor that needs to be analyzed. However, we confirmed that there was no significant differences in the 15-PGDH mRNA expression levels of normal-appearing colorectal mucosa according to age (P = 0.790).
This study has some limitations, including a small sample size and an incomplete number of follow-up examinations. Because of this small sample size, we could not perform multivariate analysis. The results of our study did not indicate a dose-response relationship between 15-PGDH mRNA expression in normal colorectal mucosa and SA burden, because our study did not include a sufficient number of samples prove conclusively this quantitative relationship. Therefore, an additional, larger study is needed to clarify this finding. Another limitation is that we only examined the relative mRNA expression of 15-PGDH using quantitative real-time PCR assays and we did not confirm protein expression. We also did not measure the exact distance between the tumor and the normal colon tissues. However, in order to more precisely investigate field effect, it would be useful to divide the adjacent mucosa that is within 1 cm of the tumor from the nonadjacent mucosa. Lastly, we were unable to control the factors that affect the detection rate of adenomas, such as the skill and experience of the practitioners who performed the colonoscopies.
In conclusion, our present analyses provide novel evidence that low 15-PGDH expression in normal-appearing colorectal mucosa is associated with a more advanced stage tumor and a more synchronous adenoma in sporadic CRC patients. Expression of 15-PGDH in normal-appearing colorectal mucosa is a useful biomarker for the prediction of sporadic synchronous adenomas and could be a potential source of field effects in the colorectal mucosa. A large prospective study on 15-PGDH and multiple genetic markers that are involved in the early stages of colorectal carcinogenesis would be invaluable for determining new biomarkers for risk assessment and the early detection of colorectal neoplasms.





 XML Download
XML Download