

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Idiopathic pulmonary fibrosis (IPF) is a progressively deteriorating lung disease of unknown etiology, characterized by fibroblast proliferation and extracellular matrix consolidation (1). Globally, the incidence of IPF has been increasing, probably due to environmental factors, an increase in the elderly population, and early diagnosis using high-resolution computed tomography (HRCT) (2, 3). IPF is often lethal for specific patient populations with a median survival of approximately 3 yr (4-7). In addition, pulmonary infections caused by various organisms can often exasperate IPF, causing a high mortality rate even among the general patient population (8-10). Therefore, infection at initial presentation or during follow-up alters the required therapeutic intervention and influences patient prognosis and duration of survival, especially within Asian countries (8-11).
Mycobacterium tuberculosis (MTB) is a relatively common cause of chronic lung infections worldwide (12). Recently, the prevalence of nontuberculous mycobacteria (NTM) infection has increased rapidly in developing countries, including Korea (13-16). In studies conducted in the 1970-90s that examined patients with idiopathic chronic interstitial lung disease, the positive culture rate for MTB was 5%-6.2% (17, 18). This incidence was 4-5 times higher than that of the general population in the same country at the same time. This indicates that IPF might establish pulmonary susceptibility to mycobacterial infection. In the case of IPF patients with NTM infection, little data are available in the literature. For example, one of the few findings that were reported is the high rate of M. fortuitum found in NTM infections among patients with underlying IPF (19). However, more comprehensive analysis of other types of NTM infections is needed for proper use of immunosuppressants in IPF. This is because the current treatment guidelines for IPF recommend steroid and immunosuppressive drugs as the main therapy (1, 20), which are expected to increase the chance of reactivation of dormant pulmonary infections and mortality caused by TB and nontuberculous mycobacterium lung disease (NTMLD).
However, to the best of our knowledge, no data exist on the prevalence or clinical manifestations of NTM infection in patients with IPF. Therefore, this study investigated the prevalence of TB and NTMLD in patients with IPF at the initial presentation and during follow-up, and evaluated the clinical courses of TB and NTMLD patients with IPF.
MATERIALS AND METHODS
Study population
In total, 795 patients with IPF were diagnosed using the criteria of the American Thoracic Society and the European Respiratory Society (20), with compatible findings on surgical lung biopsy (n = 486; 68.5%) or using radio-clinical criteria (n = 309; 31.5%) at 5 university hospitals including Soonchunhyang University Bucheon Hospital, Soonchunhyang University Seoul Hospital, University of Ulsan Asan Medical Center, Yonsei University Severance Hospital and Inha University Hospital in Korea from 1992 to 2007.
Interstitial lung diseases with known etiologies, such as collagen vascular disease (CVD), a history of drug use, or environmental exposure, were excluded. At the initial evaluation of IPF, all of the subjects underwent sputum examination for acid-fast bacilli (AFB) stain and culture for Mycobacterium. Bronchoalveolar lavage (BAL) was performed in eligible subjects. During the follow-up period, sputum was examined for AFB smear and culture when pulmonary infection was suspected, based on clinical manifestation or on the radiologic evaluation, including chest radiograph (posteroanterior view) or high-resolution computed tomography (HRCT). HRCT was performed in all patients at the time of IPF diagnosis, as well as at the time when pulmonary infection with MTB or NTM was suspected. NTMLD was diagnosed using the American Thoracic Society/Infectious Diseases Society of America consensus, based on clinical pulmonary symptoms and radiologic and microbiologic findings (15). Briefly, NTMLD was diagnosed when symptomatic patients exhibited newly developed multifocal bronchiectasis, cavitation, consolidation, or nodules as well as one of the following three microbiologic criteria: 1) at least two positive cultures from sputum; 2) one positive culture from a bronchial wash or lavage; or 3) a transbronchial lung biopsy that resulted in a diagnosis of NTM or a biopsy exhibiting mycobacterial histopathologic features and one or more positive sputum or bronchial wash. Patients were treated as recommended by the guidelines of the World Health Organization (21) and a successful cure of TB or NTMLD was defined by two separate negative sputum cultures during the last month of treatment (22).
Statistical analyses
Statistical analyses were performed using the SPSS software (ver. 14.0 for Windows). Differences in variables between groups were determined using Student's t-test. The development of pulmonary TB or NTMLD between immunosuppressant users and nonusers in the IPF cohort was compared using the chi-square test. Data are expressed as the mean ± SE. P values < 0.05 were deemed to indicate statistical significance.
RESULTS
Prevalence and demographic characteristics of TB and NTMLD in patients with IPF
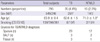
Among the 795 patients with IPF, 35 (4.4%) and 16 (2.0%) were diagnosed as having pulmonary infections with MTB and NTM, respectively. The sample sources of AFB were sputum (n = 41; 82%), bronchial wash or lavage (n = 5; 10%), and lung tissue (n = 4; 8%) (Table 1). Of the demographic features, age at IPF diagnosis was significantly older in the NTMLD group than in the TB group or for all subjects (71.0 ± 1.8 vs 62.6 ± 1.5 or 63.9 ± 0.4 yr; P = 0.006 and P = 0.005, respectively). A tendency toward a higher proportion of males was observed in the NTMLD and TB groups compared to all patients, although the difference was marginal (P = 0.057). The proportions of smokers and duration of IPF were similar between the two groups (Table 1).
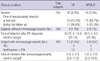
Among 35 patients with TB, 18 (51.4%) were diagnosed at the initial presentation of IPF and 17 developed TB during the followup (Table 2). A total of 16 patients were diagnosed with NTMLD: 11 (68.7%) at the initial presentation and 5 during follow-up. M. avium complex (n = 14; 88%) was the most common type of NTM, followed by M. abscessus (n = 1; 6%) and M. szulgai (n = 1; 6%). Of the 795 patients with IPF, 499 had been treated with immunosuppressants, while 296 had symptomatic treatment only (Table 2). A total of 16 of the 499 immunosuppressant users (3.2%) developed TB or NTMLD, compared to 6 of 296 (2.0%) in the symptomatic treatment group; 13 of the 499 patients on immunosuppressant therapy developed active TB compared to 4 of the 296 patients receiving symptomatic therapy (2.6% vs 1.4%, P = 0.12). Of five patients with newly developed NTMLD, three were being treated with immunosuppressants (0.6%) and two were receiving symptomatic therapy only (0.7%). Among the immunosuppressant users, the interval between the date of TB or NTMLD diagnosis and the initiation of immunosuppressant therapy was 5.8 ± 2.6 and 8.3 ± 0.2 months, respectively.
Clinical course of NTMLD and pulmonary TB in patients with IPF
The majority of new TB (76%, 13 of 17 subjects) and NTMLD (60%, 3 of 5 subjects) developed during the treatment with immunosuppressants. All patients discontinued prednisone or azathioprine after the diagnosis of mycobacterial infection and were treated with anti-MTB or -NTM chemotherapy according to the guidelines of the American Thoracic Society and the World Health Organization (21, 22). Regarding the treatment response and clinical course of TB and NTMLD, 22 (63%) of 35 patients with TB and 9 (56%) of 16 patients with NTMLD were cured (Table 3). Six and three patients in the two groups died during the anti-MTB or -NTMLD treatments, respectively. The causes of death were acute exacerbation of IPF, hemoptysis, and progression of TB (Table 3). The overall mortality rate during treatment of mycobacterial lung infection was 17.6% (9/51).
DISCUSSION
The present study showed that there was a higher prevalence of pulmonary TB and NTMLD in patients with IPF (4.4% and 2.0%, respectively). Because the prevalence of tuberculosis is 1% in the general Korean population (23), these data indicate that the incidence of tuberculosis in patients with IPF is more than four times higher than that of the general population. NTM infections, which were once regarded as contamination or colonization from the environment, are now known to be potential pathogens in certain patients. The prevalence of NTMLD has not been well documented. In industrialized countries, incidence rates vary from 1.0 to 1.8 cases per 100,000 (24). The rate of NTM lung disease is higher in immunocompromised hosts, such as those with HIV infection, diabetes, and organ transplant recipients (25-27). Furthermore, advances in diagnostic technology have facilitated the detection and identification of NTM (15). However, to date, no comprehensive data exist on NTM infections in patients with IPF. In the present study, the prevalence of NTMLD in patients with IPF was 2.0%, which we presumed to be a very high rate compared to the general population.
Structurally damaging lung diseases, such as chronic obstructive pulmonary disease (COPD), bronchiectasis, cystic fibrosis, and pneumoconiosis, increase susceptibility to NTMLD (15, 28-30). This can be explained by mechanical factors and impaired local host immunity. In vitro experiments have revealed that NTM is only able to adhere to damaged, not intact, mucosa (31). Impaired local immunity involves impaired clearance of secretions, abnormal airway surface liquids, and persistent airway inflammation (32). The pathology of IPF is primarily characterized by interstitial fibrosis, inflammation, and fibroblastic foci. In the later stages, secondary structural damage, such as parenchymal cystic change, traction bronchiectasis, and honeycomb change, develops. These structural (mechanical) changes can be attributed to impairment of local immunity leading to a more susceptible environment to MTB or NTM as demonstrated in the present study.
The prevalence of TB in patients with IPF (4.3%) is slightly lower in the present study than the prevalence reported by Chung et al. (6.2%) in Korea (18). They observed histologically (n = 2) or bacteriologically (n = 7) confirmed pulmonary tuberculosis among 143 patients with IPF. Although another single-center study reported that M. fortuitium were frequently isolated from underlying lung disease including prior tuberculosis, lung cancer or IPF (19), we did not identify M. fortuitum in the present study. The difference between these studies may be due to different numbers of patients or single-center versus multicenter designs.
In patients with IPF, about half (51%) of the TB cases were found at the time of initial diagnosis of IPF and the remaining half developed new TB during the follow-up period. In the case of NTMLD, 69% of NTMLD cases were found at the initial visit for the diagnosis of IPF. These high diagnosis rates at initial evaluation may be explained by the fact that prevalence of TB is still high especially elderly in Korea. Regarding NTMLD, most of our patients (14 of 16) have bronchiectasis or cavity due to previous TB. These lung structure changes enable more easily infect to NTM in addition to IPF. These data indicate that pulmonary TB and NTMLD should be suspected when respiratory symptoms or chest radiographs change during the follow-up.
More importantly, the majority of these patients were on immunosuppressant therapy. Immunocompromised states, such as HIV infection, malignancy, diabetes, chronic corticosteroid use and the use of TNF-α antagonists, are well-known risk factors for TB and NTMLD (33-38). The occurrence of TB in patients on immunosuppressant therapy was two times higher (2.6%) than that of those on symptomatic therapy (1.3%). During the follow-up period, 13 (81%) of 16 patients with TB and 3 (60%) of 5 patients with NTMLD had been treated with azathioprine or prednisone. The intervals between newly diagnosed TB and NTMLD after initiation of immunosuppressant therapy were 5.8 ± 2.6 and 8.3 ± 0.2 months, respectively. Considering the relatively short duration of immunosuppressant therapy before the development of TB or NTMLD, immunosuppressants may be a causal factor in the development of mycobacterial lung disease in these subjects.
It is generally recommended that patients on immune suppressants such as prednisone at a dose of over 15 mg per day for more than 1 month need a tuberculin test and should consider prophylactic treatment due to their increased susceptibility to mycobacterial infections (39). In the present study, we did not use skin or blood tests to examine latent TB before the start of immunosuppressant treatment, because of the high rate of BCG immunization in Korea (40). However, the diagnostic value of the skin or blood tests for detecting latent tuberculosis infection and the use of prophylaxis in these cases will be evaluated in patients with IPF in the future.
Pulmonary TB was cured in about two-thirds of the patients but other three patients died of TB progression. About 18% (9 of 51) of the patients died during treatment with anti-MTB or -NTM medications. Their causes of death were similar to typical causes in patients with IPF (8). Three patients who had been treated with steroids and azathioprine died of TB progression, suggesting the possibility of a rapid fatal course of TB in these patients, although the numbers were small.
Our study has some limitations. First, due to the retrospective design of the study, some IPF cohort patients might not have been examined bacteriologically in their sputum or bronchiolar lavage fluid during the follow-up period, even when they had supporting symptoms or radiological findings. Second, colonization and disease states in NTMLD were not readily distinguishable. Most patients with IPF had respiratory symptoms, such as coughing, dyspnea, and fatigue, which also occur in NTMLD. Moreover, once organisms were detected, treatment was promptly initiated without observation in these patients. Thus, in some patients, NTMLD may be more unlikely.
In summary, we found that the prevalence rates of pulmonary TB and NTMLD in a large number of patients with IPF were 4.4% and 2.0%, respectively. These rates are significantly higher than those in the general population, suggesting the need to more carefully test for TB and NTMLD in patients with IPF, not only at the initial presentation but also during the follow-up period, especially in patients being treated with immunosuppressive agents.

 XML Download
XML Download