

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Despite considerable improvement of care and outcomes of acute ST-segment elevation myocardial infarction (STEMI) in recent years, STEMI remains one of the most fatal disease in Korea as in the western and developing countries (1, 2). Because of the front wave of necrosis expanding from endocardium subtended by infarct artery, the size of infarction and mortality increases in proportion to the elapsed time after coronary artery occlusion (3, 4). Timely reperfusion of infarct related artery is the cornerstone of treatment for interrupting the progression of necrosis and salvaging myocardium (5, 6). The outcomes of reperfusion therapy are critically dependent on the ischemic time from the onset of symptoms to the treatment (7, 8).
Strategy to shorten the ischemic time involves integrated efforts to shorten the time delay in successive stages of patients' decision, transfer, and inhospital management. Recent efforts to implement the expedient reperfusion as recommended in clinical guidelines (door-to-needle time ≤ 30 min, door-to-balloon time ≤ 90 min) resulted in significant curtailment of inhospital time delay to treatment and improved clinical outcomes (9-11). However, time delay prior to hospital arrival has been largely unaffected, with little signs of change ever reported in recent years (12, 13).
Prehospital delay in patients with STEMI has been found to be an important factor of in-hospital and long-term mortality (14). Nonetheless, the magnitude of, and factors associated with prehospital time delay have not clearly identified in Korea. Accordingly, the purpose of this study was to investigate and clarify the factors related to prehospital time delay in patients with STEMI presented to the emergency department.
MATERIALS AND METHODS
Study design and subjects
Patients aged 18 yr or older who presented with acute STEMI to the emergency department of Samsung Changwon Hospital from January 2008 to December 2010 were registered for the analysis. During this time, a total of 430 consecutive patients were hospitalized. Seven patients were excluded in whom the accurate time of symptom onset could not be determined.
Data collection
Demographic, medical history and clinical characteristics were registered from the hospital records by trained physicians and nurses. Educated nurses gave a person-to-person call to patients or their family members and interviewed to ask questions enlisted in questionnaire and variables difficult to get from hospital records. Clinical as well as socioeconomic variables were investigated with regard to age, sex, characteristics of symptoms, time of symptom onset, activity at the time of onset, location of residence, level of education, attendance of family member or bystanders, knowledge about myocardial infarction, the first reaction of patient to initial symptom, means of transportation, and triage via other hospitals. Patients were divided into two groups according to prehospital time delay; short delay group in whom time from symptom onset to hospital arrival is 180 min or less, and long delay group in who the time is more than 180 min.
Definitions
STEMI was defined according to the criteria of the universal definition of myocardial infarction (15). Crushing chest pain persisting longer than 20 min with or without diaphoresis was classified as typical symptoms, while other symptoms like shortness of breath, epigastric pain, nausea, and loss of consciousness were classified as atypical symptoms.
Symptom onset-to-door time was the time from the onset of symptoms to the arrival at the emergency department, and constitute a prehospital delay.
Statistical analysis
Categorical variables were summarized by counts and relative frequencies; numeric variables, by their median and range. Differences in patients' sociodemographic and clinical characteristics were compared between subgroups with chi-square test for categorical variables and Student t test for continuous variables. Overall survival was estimated using the Kaplan-Meier product limit method and differences in survival between groups were assessed by the log rank test. The logistic regression model was employed to identify the significant independent prognostic factors affecting response (symptom onset-to-door time). The multivariate model was created using a backward elimination method, and the probability was set at 0.05 for removal. Crude and adjusted odds ratios (OR) and 95% confidence interval (CI) were calculated. P values lower than 0.05 were considered statistically significant. This was a retrospective study therefore alpha was not adjusted for multiple testing. All statistical analyses were carried out using SPSS version 14.0 and MedCalc version 11.6.1 statistical software (SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics of study subjects
Baseline characteristics of 423 study patients are shown in Table 1. The mean age was 61.6 ± 13.0 yr, and 73% of the patients were male. Of all patients, 87% (n = 369) were eligible for thrombolysis or primary percutaneuous coronary intervention (PCI). Acute reperfusion therapy was performed in 95% of these patients (thrombolysis, 12 patients [3%]; primary PCI, 340 patients [97%]) (Table 2). The patients in the short- and long delay groups did not differ with respect to the demographic characteristics, social and past medical history, except for diabetes where the prevalence was higher in long delay group than in short delay group (30% vs 21%, P = 0.038).
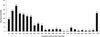
The mean symptom onset-to-door time of total 423 patients was 255 ± 285 (median: 150) min. Of the study groups, 337 patients (79.7%) arrived at the hospital within 6 hr of symptom onset and only 28 patients (6.6%) arrived within 30 min of symptom onset, a goal recommended in the recent guidelines (16) (Fig. 1).
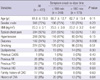
The sociodemographic characteristics are presented in Table 3. Seventy-six percent of overall patients enrolled in this study was referred from other hospital or clinics. Among sociodemographic variables, low educational level, triage via other hospital, use of private transport, and symptom-onset during night time (6 pm-6 am) were more frequently observed in long delay group. Age, gender, characteristics of symptoms, previous ischemic heart disease (IHD), residential area, knowledge about acute myocardial infarction (AMI), and patients' responses to symptoms were not different between two groups.
Factors related to prolonged prehospital delay
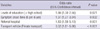
In univariate analysis, body mass index (BMI), history of diabetes, levels of education, symptom-onset-time, triage via referral hospital and use of private transport were significantly associated with prehospital delay (Table 4). By multiple logistic regression analysis, low levels of education (< high school), symptom onset during night time (6 pm-6 am), triage via other hospital and use of private transport were statistically significant factors associated with prehospital delay (Table 5).
Clinical outcomes according to prehospital delay
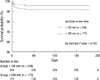
Nineteen patients (4.5%) had died during the admission (Table 6). Inhospital mortality was significantly higher in long delay group compared with short delay group (12 [6.9%] vs 7 [2.8%], P = 0.048). Mortality at 30 days and 6 month was also higher in the long delay group, but the difference was not statistically significant (10 [4.2%] vs 14 [8.1%], P = 0.092; 17 [6.3%] vs 17 [9.9%], P = 0.178, respectively) (Fig. 2). On Kaplan-Meier analysis the survival at 6 month was similar between two groups (Fig. 3).
DISCUSSION
In the reperfusion era, the outcomes of STEMI critically depend on the total ischemic time from the onset of symptom to treatment (7, 8). Prehospital delay is an important determinant of total ischemic time, yet unlike inhospital delay, it is difficult to employ systematic approach to reduce the delay substantially. Therefore, prehospital delay remains largely unchanged over recent years in spite of the notable improvement in reducing time delay in the hospital after patient's arrival (9-13).
The result of this study showed that in the typical Korean community comprised of a large city and surrounding suburban area, the time from symptom onset to hospital arrival was still too long for optimal management of the patients with acute STEMI. Prehospital time delay in this study (mean 255 ± 285 min; median 150 min) already exceeded the goal of total ischemic time 120 min (16). It has not been improved from earlier data of regional community in which median prehospital time delay was 172 min and also similar to previous nationwide registry data (17, 18). Although 79.7% of study patients arrived at the hospital within 6 hr of symptom onset, only 6.6% of the patients arrived within 30 min of symptom onset, which is the goal of the recent guideline for the optimal reperfusion (16).
It was noticeable that only 7% of study patients both in short and long delay group were aware of the possibility of acute MI. This might have deterred the patient's prompt action to call for help, and accounted for much of the delay. In addition, about 30% of the patients were using private transport to arrive at a hospital, and 76% of the patients were transferred via other hospital, contributing to delayed presentation. These data suggest that a nationwide and/or local-based coordinated effort is required to enhance public awareness for risk of STEMI and to build an efficient emergency dispatch system.
To find the factors that correlate with delayed hospital arrival, patient-related factors and sociodemogrpahic factors were sought in the study population. Multivairate logistic regression revealed that patient's level of education, symptom onset during night time, arrival via other hospital, and use of private transport were significant determinants for prehospital time delay. These findings differed from previous report that old age, female gender, diabetes, hypertension, previous history of coronary heart disease or coronary intervention were associated with prolonged prehospital delay (19-23). Relatively small sized study population, and low incidence of previous coronary disease in the present study may have reduced the power to discriminate the risk among the patients. Remarkably, low level of education (not completing high school) was significant factor for prehospital delay (hazard ratio 1.66) in this study. Shorter time of education has been also shown to increase the delay in an Australian study (24). It is conceivable that low level of patient education elicited slower reaction of patients, or it just might mirror the low socioeconomic status, which has been shown to be related to time delay (25). Night time onset and arrival via other hospitals were another factors, which was understandable and concurred with other study (17, 26). Most strongly associated with time delay was use of private transport as opposed to ambulance (hazard ratio 3.02), although the rate of private transport decreased considerably compared with previous regional community study in Korea (17). The cause of this relation is difficult to define, but private transportation may be accounted by other factors, such as low level of education or the lack of patient's perception of urgency. Prehospital triage by the emergency medical service should be encouraged because it is associated with a shorter time to treatment and more favorable clinical outcomes (27).
In this study, inhospital mortality was significantly higher in long delay group compared with short delay group. During the period of 30 days and 6 months follow-up, the mortality benefit of short treatment delay was continuously observed, although the differences were not statistically significant. Of the study patients eligible for reperfusion therapy, 340 (92%) of 369 patients were treated with primary PCI and the above result was consistent with previous report that treatment delay is critical determinants of outcomes after primary PCI (3). Several studies, mostly observational ones including Korean registry, have suggested that the time dependency of reperfusion effect was less pronounced in the setting of primary PCI than in fibrinolysis (18, 28, 29). However, the concept of "time-insensitivity" of primary PCI has been recently questioned because of the confounding factors associated with observational data (30). Therefore, although the role of primary PCI as a better reperfusion strategy is valid, the importance of reducing time delay should be applied to primary PCI, too.
Several limitations of this study warrant consideration. Firstly, the number of the patients in this study was relatively small. This might have deprived the power to detect the association between several variables and the time delay. Secondly, this study was retrospective, based on the information in the hospital medical records and interviews with patients and their family members, which could have been affected by recall bias. Finally, initial means of transportation and times between visiting first hospital and arriving in emergency department were not evaluated because of inaccurate information from referring hospitals. Despite the limitations, the present study could provide the descriptive data showing the current status of triage for emergency management of STEMI patients.
In conclusion, the present study demonstrated significant prehospital delay in the treatment of STEMI patients in Korean community and the delay was correlated with inhospital mortality. In Korean STEMI patients, low educational level, symptom onset during night time, triage via other hospital and private transport are associated with the treatment delay. Public campaigns, education and counseling of patients and their families are needed to raise the public awareness of STEMI that should prompt to seek immediate medical attention for optimal patients' outcomes.




 XML Download
XML Download