

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Non-specific interstitial pneumonia (NSIP) has been proposed as a histological subtype of idiopathic interstitial pneumonia and is characterised by varying degrees of alveolar wall inflammation and fibrosis in a pattern that suggests temporal homogeneity (1). NSIP is associated with various medical conditions such as human immunodeficiency virus infection, hypersensitivity pneumonitis, and several collagen vascular diseases (CVDs) including polymyositis-dermatomyositis, rheumatoid arthritis, Sjögren's syndrome, and systemic sclerosis. The diagnosis of idiopathic NSIP is made when no specific cause can be detected (1-7).
The overall prognosis and response to steroid therapy is generally favourable in patients with NSIP (1, 8-12). However, not all patients respond well to treatment. In some patients, relapse can occur when steroids are tapered or stopped. In others, steroids do not modify disease activity, leading to disease progression and death. Travis et al. (9) suggested that separating the cellular from the fibrotic patterns of NSIP is important because survival might differ between these two groups. Patients with cellular pattern NSIP have 5- and 10-yr survival rates similar to those with desquamative interstitial pneumonia, whereas those with fibrotic pattern NSIP have a worse 5-yr survival rate, which was similar to those with usual interstitial pneumonia (9). Park et al. (13) also reported that patients with fibrotic NSIP are frequently hospitalised with a recurrence rate of 36%. However, there are relatively few data on the clinical course and outcomes other than mortality. It is also unclear which factors affect the responsiveness to steroids and relapse.
The purpose of this study was to investigate the clinical course of NSIP after treatment and to determine which factors are associated with the responsiveness to steroids and relapse.
MATERIALS AND METHODS
Study subjects
We reviewed the medical records of patients admitted to a tertiary referral hospital (Seoul National University Hospital) from March 1995 to July 2007. We found 41 patients who were diagnosed clinically with NSIP at discharge who had undergone a surgical lung biopsy for a histological examination. The biopsy slides were reviewed by three pathologists according to the American Thoracic Society/European Respiratory Society consensus classification of interstitial pneumonia (14); and 37 patients with pathologically confirmed NSIP were selected. We excluded two patients lost to follow-up, so 35 patients were included.
Variables and definitions
A retrospective study was performed to identify factors associated with the responsiveness to steroids and relapse. Clinical, radiological, and laboratory data were reviewed, including age, gender, smoking history, symptoms on admission, comorbidities, initial oxygen tension in arterial blood (PaO2), results of pulmonary function tests, and steroid doses.
The response to steroid was assessed from the clinical records of the patients and included improvement in symptoms, radiographic findings, and pulmonary function tests (PFTs) after initial corticosteroid therapy. The timing for assessing the response was 1 yr after the initiation of treatment. Improvement was defined as > 10% increase in forced vital capacity (FVC) and diffusing capacity of the lung for carbon monoxide (DLCO). Progression was defined as > 10% decline in FVC and DLCO from baseline and/or death. When the PFT data could not be obtained because of worsening of respiratory symptoms accompanied by continued worsening of findings on chest radiography (e.g. acute exacerbation), the case was also defined as disease progression. Patients who did not demonstrate improvement or progression were considered stable. Finally, we classified the patients who showed improvement or remained stable after the initial steroid therapy as steroid responders, and those who showed progression as steroid non-responders.
Relapse was defined as an aggravation of symptoms and lung function (and/or radiological abnormalities) after complete discontinuation of treatment and treatment with prednisolone and/or cytotoxic agent was restarted.
Analysis
Continuous variables were analysed in the univariate analysis using non-parametric tests (Mann-Whitney U- or Kruskal-Wallis tests), and categorical variables were compared using Pearson's chi-squared or Fisher's exact test, as appropriate. Survival was evaluated using the Kaplan-Meier method. A survival analysis was performed on the total sample, including patients with cellular or fibrotic NSIP, because the number of patients was small, only three deaths occurred, and the histological subtypes could not be distinguished in many patients. SPSS version 17.0 (Chicago, IL, USA) was used for all analyses. A P value < 0.05 was considered significant.
RESULTS
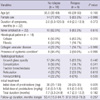
Twenty-eight women and seven men (median age, 52 yr) were included in the analysis. The demographic and clinical characteristics of the enrolled patients are described in Table 1. Most patients presented with subacute onset of dyspnea or cough. Ground-glass opacity was the most frequent abnormality (88.6%), followed by consolidation (40.0%) on the initial chest computed tomography (CT) scans. A histological analysis showed the cellular pattern in 17 patients (48.6%) and the fibrotic pattern in 10 patients (28.6%); the histological NSIP subtype was indeterminate in eight patients (22.9%). The median follow-up duration for survivors was 55.2 months (range, 15.9-102.0 months).
The follow-up results of the enrolled patients are summarised in Fig. 1. All 35 patients received corticosteroid therapy alone as the initial treatment, and cytotoxic agents were added in seven patients (four patients cyclophosphamide; three patients azathioprine) who showed rapid disease progression or steroid dependency. The median dose of initial prednisolone was 0.54 mg/kg/day. A higher dose of initial steroids (> 1.5 mg/kg/day) was used in only two patients, 9.5 mg/kg/day in one patient who showed rapid disease progression, and 1.8 mg/kg/day in another who showed arterial hypoxemia on room air (PaO2, 54.3 mmHg). The range of initial prednisolone doses used in patients except these two was 0.4-1.1 mg/kg/day. The prednisolone dose was slowly tapered after 4-6 weeks based on the clinical and PFT evaluation of early response. Thirty (86%) patients responded to steroid therapy, and five (14%) were considered non-responders. Three of the 5 non-responders died of disease progression with combined pneumonia, although all had received additional cyclophosphamide pulse therapy. The patients died 1.6, 1.7, and 5.2 months after beginning treatment. In contrast, steroid responders were all alive at the end of the follow-up period. Six (20%) steroid responders were stable but were considered steroid dependent because the disease worsened when steroids were reduced. Therefore, steroid treatment was maintained in these six patients for the entire follow-up period, and azathioprine was added in two patients. The maintenance dose of prednisolone was 5 mg in five patients and 15 mg in one patient. The 1- and 5-yr survival rates in all patients were 97.1% and 93.9%, respectively.
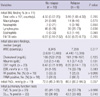
Table 2 shows a comparison of various parameters between steroid responders and non-responders. Histological subtype was not related to steroid response. Smoking history, period from the onset of symptoms to treatment, initial chest CT findings, initial PFT results, and initial bronchoalveolar lavage findings did not differ between the groups. However, seropositivity for the fluorescent antinuclear antibody (FANA) was significantly associated with a poor response to steroids. Higher erythrocyte sedimentation rate (ESR) tended to be related to disease progression. Table 3 shows the clinical characteristics of steroid non-responders. Most of the patients with poor treatment outcomes had underlying systemic conditions associated with NSIP, such as CVD or exposure to drugs.
Twenty-four (80%) of the 30 steroid responders showed clinical improvement after initial treatment, and 18 (75%) remained relapse free during the median follow-up of 41.5 months (range, 5.1-76.4 months) after discontinuing the steroids. Relapses occurred in six (25%) of 24 patients within a median of 8.2 months (range, 3.0-16.4 months) after withdrawal of steroids. Patients who relapsed were all retreated with a median steroid dose of 30 mg (range, 25-30 mg), and azathioprine was added in one patient. The median duration of retreatment was 4.3 months (range, 3.5-10.7 months) in four patients, and steroid treatment was maintained in another two patients. Patients with and without relapse were compared to search for predictive factors (Tables 4 and 5). The initial dose of prednisolone was significantly lower in the relapse group. Additionally, the duration of initial treatment tended to be shorter in the relapse group (4.7 vs 7.7 months), but no statistical significance was observed. Smoking history, histological pattern, presence of CVD, initial chest CT, and PFT and laboratory findings did not differ significantly between the groups. The detailed lists of underlying systemic conditions in steroid responders are summarized in Tables E1 and E2.
Both FVC and DLCO improved gradually in both the cellular and fibrotic NSIP groups. DLCO tended to be higher in patients with cellular NSIP than in those with fibrotic NSIP throughout the follow-up period, although the difference was not significant. A comparison of the PFT results between patients with and without CVD showed that FVC and DLCO tended to be lower in patients with CVD than in those without CVD but without statistical significance. Patients with CVD tended to have fewer changes in PFT results, however this difference was not significant (data not shown).
DISCUSSION
The NSIP population showed clinical similarities to previous study populations with a predominance of never-smoking, middle-aged females (15, 16). In our study, the overall prognosis of patients with NSIP was generally favourable with an initial response rate to steroid therapy of 86% and a 5-yr survival rate of 93.9%. The overall 5-yr survival rate varied in previous studies (1, 3, 8, 17-19); and this variation could be explained by the heterogeneity of the populations studied in terms of histological subtypes and the underlying conditions associated with NSIP. The survival rates in our study were higher than those reported previously in patients with fibrotic NSIP but were lower than those in patients with cellular NSIP (3, 9, 13, 18).
The presence of an underlying systemic condition might be relevant to a poor prognosis for patients with NSIP. Notably, all five patients in the progression group had chronic diseases or associated conditions such as CVD and sustained exposure to drugs or chemicals. Among the three patients who died, one had dermatomyositis and Sjögren's syndrome and another had a history of sustained exposure to paint fumes for > 40 yr. Another patient had acute lymphoblastic leukaemia and had been treated with imatinib for about 15 months before NSIP was diagnosed. She died of progressive NSIP, although complete remission of leukaemia had been achieved. FANA seropositivity was also significantly associated with progression, and the initial ESR level tended to be higher in the progression group. Anti-nuclear antibodies are found in patients not only with autoimmune diseases but also those with various non-rheumatological conditions associated with tissue damage such as infections, cancer, and hormonal or blood diseases. Recent studies have shown that even idiopathic NSIP might be associated with an autoimmune background that later reveals itself as an organspecific or a systemic autoimmune disease (20, 21). Thus, we presumed that the presence of ANA might be an early manifestation of this systemic background and that simultaneous systemic manifestations might be related to a poor prognosis. This possibility parallels our results showing the patients with NSIP and various systemic conditions had worse prognoses. Unfortunately, we found no statistically significant relationship between the systemic conditions and poor prognosis for NSIP, probably because of the small sample size and the heterogeneity of associated conditions. The pathophysiological responses to injury grade might differ between patients with various conditions associated with NSIP. Felício et al. (22) detected significantly greater collagen and elastic fibre proliferation in the lungs of patients with CVD and NSIP compared with those with idiopathic NSIP. The increased elastosis may have been caused by major repair and remodelling processes following septal inflammation and consequent fiber fragmentation. These processes might also be responsible for the loss of the normal alveolar wall architecture, which contributes to alveoli collapse, thereby impairing the mechanisms of inflammatory resolution (22). Recently, a case series of progressive NSIP revealed a change in histology to a more fibrous pattern through sequential biopsies, and half of the patients had CVD (23). Progression of fibroproliferation is associated with poor outcomes in response to steroid treatment (24).
Among the steroid responders in our study, up to 40% of patients suffered relapse or steroid dependency. Park et al. (13) reported that relapse occurred in 36% of patients with fibrotic NSIP who improved or were stable after initial treatment, and the disease-related mortality was 30% in this subgroup. In contrast, all of the relapsed patients in our study showed improvement after re-treatment with steroids, and none of the patients in this subgroup died. We also found that a lower dose of initial steroid was associated with a relapse of NSIP, a finding that contrasts with that of Park et al. (13). However, the initial doses of steroid in the study by Park et al. (13) were higher than the doses used in both the relapse and no relapse groups in our study. The study by Park et al. (13) included only patients with fibrotic NSIP, whereas we included both cellular and fibrotic subtypes in the analysis of relapse. The optimal dose and duration of glucocorticoid therapy is still unclear because most studies of patients with NSIP used a variety of regimens in a small number of patients (8, 13, 19, 22, 24, 25).
This study had some limitations. First, it was a retrospective study with a small sample size, so a multivariate analysis could not be performed. Second, the pathological subtypes could not be confirmed in all patients, although we attempted to identify the pathological patterns in all patients. Third, a possibility of selection bias existed between the biopsy group and the non-biopsy group in patients with CVD and NSIP. Surgical biopsy was performed in most patients with atypical radiological features other than usual interstitial pneumonia. However, we believe that it is difficult to make a correct clinical diagnosis of the various types of CVD based solely on CT findings (26). Finally, our study population included a heterogeneous group with various underlying conditions associated with NSIP.
In conclusion, we investigated the treatment course of NSIP and identified several prognostic factors for treatment response and relapse. In patients who show sustained disease progression despite treatment, the progression is associated with various systemic conditions such as CVD, malignancy, or exposure to drugs or chemicals. A lower dose of initial steroids is significantly associated with relapse.




 XML Download
XML Download