

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Most of ingested foreign bodies pass through the gastrointestinal tract uneventfully within a week. However, symptoms may arise due to occasional obstruction or perforation (1). Commonly reported foreign bodies include toothpicks, fish bones, and chicken bones. These objects and long, narrow, or pointed foreign bodies are associated with a high risk of impaction and perforation of the bowel walls (2, 3).
The ingestion of foreign bodies may also lead to penetrating injuries with complicating abscess formation. The patients in these cases tend to not recall the specifics of the ingestion. Symptoms are nonspecific, and foreign bodies may not be obvious on plain films, ultrasounds, or computed tomographic images. Patients may also give vague or non-specific information, making it difficult for clinicians to determine proper treatment.
We present herein a patient who underwent surgery to rule out a primary omental tumor, an impression that had been suggested by radiologists based on the results of multiple diagnostic modalities. We were not then aware that the patient had eaten the Korean delicacy "Kanjang-gaejang," which is raw crab seasoned with soy sauce. A crab leg was found during surgery, and the patient was diagnosed with an antral perforation with abscess formation in the omentum due to foreign body migration.
CASE DESCRIPTION
A 59-yr-old man presented to the emergency department complaining of continuous epigastric and right upper quadrant pain for the previous 3 weeks on 23th March, 2009. He had no history of hypertension or diabetes. He had smoked one pack of cigarettes every day for 40 yr and was a social drinker. He did not have any changes in bowel habit or hematochezia. The patient had undergone a gastrofiberoscopy and colonoscopy 20 days earlier in a local clinic. Endoscopic findings had revealed chronic gastritis and a polyp in the colon. Fatty liver had also been reported on the abdominal ultrasonography.
The patient had the persistent abdominal pain worsened during the last 3 days. He had focal rigidity and tenderness in the right upper quadrant of his abdomen. His initial vital signs were: blood pressure 110/60 mmHg, pulse rate 88/min, respiratory rate 20/min, and temperature 36.3℃. Six hours after presentation, he complained of chills with a high body temperature of 38.0℃. The complete blood count showed a white blood cell count of 16,800/µL, hemoglobin concentration of 14.1 g/dL, and platelet count of 350,000/µL. Blood chemistry data revealed severe increases in C-reactive protein (346 mg/L) and erythrocyte sedimentation rate (55 mm/hr), with mildly elevated levels of aspartate aminotransferase and alanine aminotransferase (127 and 175 IU/L). Bilirubin, albumin, and other blood component chemistries were all within the normal range.
Plain radiographs of the chest and abdomen were unremarkable. Pre-contrast and contrast enhanced computed tomography (CT) showed an approximately 6.0 cm, ill-defined heterogeneous enhancing hypodense mass lesion in the gastrocolic ligament (Fig. 1). The mass extended to its peripheries, with ill-defined infiltration of the surrounding omentum. Radiologists called for further workup to differentiate among metastatic mass, primary omental tumor, and omental infarction.
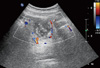
Viral and tumor markers, including carcinoembryonic antigens, alpha-fetoproteins, CA 19-9, and CA 125, were within normal ranges. Gastroduodenoscopy and colonoscopy showed simple chronic gastritis. Abdominal ultrasonography displayed an ill-defined, heterogeneous echogenic mass between the stomach and transverse colon (Fig. 2). Further imaging with positron emission tomography CT revealed a large intense hypermetabolic mass in the gastrocolic ligaments without evidence of metastasis. An exploratory laparotomy was consequently performed under the impression of necrotic tumorous lesion.
The operative field revealed a 4-cm crab leg embedded within the approximately 6-cm abscess in the perforated antrum of the stomach (Fig. 3). Streptococcus sp. was cultured from the abscess. The patient underwent antrectomy, vagotomy, and transverse colon wedge resection. A detailed history taken after surgery uncovered the Kanjang-gaejang ingestion three weeks before, one day prior to the onset of abdominal pain. Twenty days after admission, the patient was discharged from the hospital with no complications.
DISCUSSION
Foreign body ingestion is frequently encountered in emergency departments. Management of this situation depends on the nature of the material ingested. Sharp objects carry the risk of perforation, while toxic materials, such as button batteries, may need emergency endoscopic extraction. Less than 1% of ingested foreign bodies perforate the gastrointestinal tract, and most foreign bodies pass through the gastrointestinal tract within one week without any complications. When perforation does occur, the most commonly involved areas are the duodenum, ileocecal, and rectosigmoidal regions (1, 4, 5).
Ingested foreign bodies mostly cause non-specific symptoms. However, when ingestion is accompanied by intra-abdominal perforation, patients may present with abdominal pain (95%), fever (81%), or localized peritonitis (39%). Several studies report complications that include liver abscess, deep neck infection, and thyroid abscess (6, 7).
Abdominal ultrasonography and CT scans are the preferred diagnostic modalities in such cases. An endoscopy may also be helpful if performed before the foreign body migrates and the mucosa starts to heal. The high density lesion in the pre-enhanced and contrast enhanced phases of the abdominal CT in our patient could have been the foreign body. Free pneumoperitoneum is rare as the foreign body is gradually impacted and the perforation is locally covered with fibrin (1, 8).
Our patient did not initially recall the ingestion and had non-specific symptoms and laboratory results. Ultrasonography and CT showed a pseudotumorous lesion mimicking an omental tumor in the gastrocolic ligament. Unaware of the ingestion history, clinicians and radiologists placed priority on malignant necrotic lesions. The migrating foreign body had remained unproblematic until forming an abscess in the gastrocolic ligament. This rare circumstance further complicated the diagnosis.
Mass lesions of the omentum may originate from omental tumors, such as sarcoma and mesenteric embryoma, as well as from omental hernias, infarctions, or abscesses. Primary omental tumors and abscesses are rare. Non-neoplastic omental tumors are rare and include hamartomas, cryptococcosis, inflammatory pseudotumors, and foreign body granuloma. Primary omental abscesses with unknown etiology are also very rare. They tend to be male dominant and develop adjacent to the transverse colon (6, 9).
Commonly ingested foreign bodies vary by country and depend on dietary habits. Fish is a major part of the Japanese diet, and there are numerous reports of bowel perforation caused by fishbone in the Japanese literature (5). However, no previous case of bowel perforation from eating crab legs has been published to date. Koreans sometimes chew and swallow the crabs whole instead of spitting the shells out. Crab leg ingestion should not be overlooked as a possible cause of bowel perforation and abscess formation in patients with unexplained abdominal pain.
A solitary foreign body granuloma or pseudotumor can be difficult to diagnose without the appropriate history. This case demonstrates that, in the absence of a reliable history, the migration of an ingested foreign body into the intraabdominal omental area may result in chronic inflammation, a silent clinical course, and radiologic features suggestive of a neoplasm.


 XML Download
XML Download