

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) are life-threatening clinical syndromes characterized by severe inflammation in the lungs. Clinical conditions such as pneumonia, sepsis, aspiration, severe trauma, multiple transfusions, and cardiopulmonary bypass are known to be associated with the development of ALI/ARDS (1).
Host immune system plays important roles in pathophysiology and outcome of ALI/ARDS. Dysregulated systemic inflammation influenced by multiple host factors causes persistent elevation of circulating inflammatory cytokines and chemokines, which is responsible for multiple-organ dysfunction syndrome as well as the progression of ALI/ARDS (1-3). The existing reports about ALI/ARDS are mostly based on adults with various underlying medical conditions which can influence final outcomes.
Previous researches show that the increased coagulant activity and attenuation of fibrinolysis are pathologic features (1, 4, 5) reflecting the severity and prognosis (6) of ALI/ARDS in adults. However, this topic is rarely investigated in pediatric patients.
In this study, we analyzed medical records of children with ALI/ARDS to find out the relation between laboratory values indicating coagulopathy and the outcome of patients.
MATERIALS AND METHODS
Patient selection
We retrospectively analyzed the medical records of 83 children who were diagnosed as acute lung injury (ALI) or acute respiratory distress syndrome (ARDS) in the pediatric intensive care unit of Seoul National University Children's Hospital between January 2008 and December 2009. Four patients who were diagnosed as hepatic failure before the onset of ALI/ARDS were excluded because, in general, hepatic failure causes coagulopathy irrelevant to the influence of ALI/ARDS.
All the patients were intubated and received mechanical ventilation. Mortality rate was 59% (n = 47).
Definitions
ALI and ARDS were defined as the PaO2/FiO2 ratio < 300 torr and < 200 torr, respectively, with the presence of bilateral alveolar infiltrates on the chest radiograph without evidence of left ventricular failure (7). Oxygenation index (8) (OI; FiO2 × mean alveolar pressure × 100/PaO2) and ventilation index (9) (VI; respiratory rate × ([peak inspiratory pressure - positive end-expiratory pressure] × PaCO2/1,000) were used to stratify patients into the lower and higher severity groups.
Sepsis was defined according to guidelines from International Pediatric Sepsis Consensus Conference: the presence of signs of systemic inflammatory response syndrome (fever or hypothermia, tachycardia, tachypnea, and leukocytosis or leukopenia) plus suspected or proven infection (10). The Pediatric Risk of Mortality (PRISM) III score, which is a physiology-based scoring system for mortality risk based on variables including blood pressure, consciousness, and various laboratory values, was assessed using parameters including most abnormal values obtained during the first 12 hr of stay in the pediatric intensive care unit (11).
The overall survival rate (OS) was defined as cumulative rate of survival from the onset of ALI/ARDS. The failure-free survival rate (FFS) was defined as cumulative rate of survival without coexistent non-pulmonary organ failure which had occurred after the onset of ALI/ARDS. Coexistent organ system failure was defined as failure of major organs other than the lung (e.g., brain, liver, or kidney) occurred between the onset of ALI/ARDS and 24 hr prior to death. Any organ system failure occurred within 24 hr prior to death was considered as a death-related process.
Coagulation variables
Biomarkers including prothrombin time (PT), activated partial thromboplastin time (APTT), fibrin degradation product, D-dimer, antithrombin III, and platelet count obtained within 24 hr from diagnosis of ALI/ARDS were analyzed as parameters indicating coagulopathy.
Statistics
Two-sample Kolmogorov-Smirnov test was used to compare means. Kaplan-Meier analysis was used for evaluation of the cumulative rate of survival. Cox proportional hazards regression model was used for multivariate analysis of survival. The statistical analysis was performed using Statistical Package for the Social Sciences software version 17.0. Results were considered to be statistically significant when P values were less than 0.05.
RESULTS
Patient characteristics
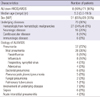
Total number of patients was 79. The age of patients at the onset of ALI/ARDS ranged 0.0-19.5 with a mean of 6.5 yr. Twenty-three patients (29%) were less than 2 yr old, 19 (24%) were 2-5 yr old, 26 (33%) were 6-12 yr old, and 11 (14%) were 13 yr old or more.
Eight (10%) and 71 (90%) patients were diagnosed as non-ARDS ALI (200 ≤ PaO2/FiO2 < 300 torr) and ARDS (PaO2/FiO2 < 200 torr), respectively. Fifty-one patients (65%) were male. Seventy patients (90%) had underlying diseases. The most common underlying disease was hematologic malignancy (n = 27, 34%). Forty-two (53%) patients were categorized into immunecompromised hosts due to malignancy (n = 33, 42%), immunologic diseases (n = 6, 8%), or previous immune-suppressive therapy (n = 3, 4%).
The most common etiology of ALI/ARDS was pneumonia (n = 57, 72%). In 42 patients (53%), organisms responsible for respiratory infection were detected in transtracheal aspirates by culture or polymerase chain reaction analysis (Table 1).
Treatment for ALI/ARDS
Seventy-six (96%) patients received antibiotic agents with or without evidence of bacterial infection. Thirty-seven (47%) patients received systemic corticosteroids for treatment of ALI/ARDS (n = 25, 32%), as chemotherapy against coexistent malignancy (n = 7, 9%), or for other reasons.
Treatment for coagulopathy after ALI/ARDS
Transfusion of fresh-frozen plasma (FFP), cryoprecipitate, and platelet were done in 60, 8, and 49 patients (79, 10, and 62%), respectively. Among 37 patients with proglonged PT (≥ 1.46 international normalized ratio, INR), 36 received either transfusion of FFP or replacement of vitamin K, or both. Replacement of antithrombin III and vitamin K after the diagnosis of ALI/ARDS were done in 43 and 56 patients (52 and 67%), respectively.
Among the 13 patients who received transfusions of FFP within 72 hr prior to diagnosis of ALI/ARDS, 2 patients with PT < 1.46 INR and 3 patients with APTT < 50 were excluded from the survival analysis considering the effect of transfused FFP on PT or APTT. Two patients who received antithrombin III within 72 hr prior to the diagnosis of ALI/ARDS were excluded from the survival analysis.
Survival
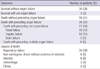
The cumulative overall survival rate (OS) and non-pulmonary-organ-failure-free survival rate (FFS) were 37% and 35%, respectively (Fig. 1). Thirty-two patients were alive for 0-29 months (mean, 13; median, 14) after the diagnosis of ALI/ARDS. The mean and median values of time from the onset of ALI/ARDS to death were 37 and 14 (0-378) days, respectively. The most common cause of death was respiratory failure (30 of 47, 64%) which was directly related to ALI/ARDS (Table 2).
Three patients had organ failure which had occurred before the onset of ALI/ARDS. Among them, one patient with pre-existing bone marrow failure died of respiratory failure and the other one with pre-existing renal failure died of sepsis. Another one patient with pre-existing renal failure survived.
PT was normal (≤ 1.20 INR) in 10 of 29 survivors (34%) and 7 of 45 non-survivors (16%). APTT was normal (≤ 35 sec) in 5 of 29 survivors (17%) and 6 of 45 non-survivors (13%).
Variables associated with survival by univariate analysis
OI, VI, and PRISM III score were higher in survivors than in non-survivors. PT and APTT were prolonged in non-survivors than in survivors. Fibrinogen, antithrombin III, and platelet count were lower in survivors than in non-survivors (Table 3).
Patients were grouped by variables which showed association with survival by univariate analysis. Cut-off value of each variable was obtained using receiver operating characteristic (ROC) curve: PRISM III score, 10 (lower, n = 23, 29%; higher, n = 53, 67%); OI, 14.5 (n = 32, 41%; n = 47, 59%); VI, 40 (n = 40, 51%, n = 34, 43%); PT, 1.46 INR (n = 35, 46%; n = 38, 48%); APTT, 50 seconds (n = 36, 46%; n = 38, 48%); fibrinogen, 375 mg/dL (n = 52, 63%; n = 24, 30%); antithrombin III, 74% (n = 33, 42%; n = 11, 14%); and platelet count, 155 × 103/µL (n = 19, 24%; n = 34, 43%).
Underlying diseases, immune state, administration of corticosteroids, transfusion, coexistent sepsis, fibrin degradation product, and D-dimer did not show association with survival.
Variables associated with survival by multivariate analysis
For multivariate analysis, patients were stratified by OI (< 14.5, ≥ 14.5) or VI (< 40, ≥ 40). The cut-off values were determined by univariate analysis as mentioned above.
In multivariate analysis with stratification by OI, prolonged APTT (≥ 50 sec) was independently associated with lower OS (hazard ratio, 95% confidence interval; 2.062, 1.031-4.121). In stratification of patients into different VI groups, prolonged PT (≥ 1.46 INR) (2.232, 1.095-4.540) and prolonged APTT (2.574, 1.230-5.386), and lower platelet count (≤ 155 × 103/µL) (3.008, 1.022-8.851) were associated with lower OS.
In stratification of patients into different OI groups, prolonged PT (2.043, 1.027-4.064) and prolonged APTT (2.422, 1.227-4.781) were associated with lower FFS. In stratification of patients into different VI groups, prolonged PT (2.177, 1.092-4.342) and prolonged APTT (3.089, 1.500-6.360) were associated with lower FFS (Table 4).
DISCUSSION
Activation of coagulation and extravascular fibrin deposition in the alveolar compartment by interrelationship between inflammatory mediators and coagulation cascade are known to be associated with pathogenesis of ALI/ARDS (1). Tissue factor combines with activated factor VII, which initiates local coagulation via the extrinsic pathway, resulting in the formation of fibrin. Alveolar fibrin membranes inactivate surfactant and disturb gas exchange. Organization and remodeling of fibrin contribute to alveolar fibrosis (6).
Previous researches show that the severity of coagulopathy is associated with mortality in patients with ALI/ARDS. McClintock et al. analyzed 50 adults with ALI and reported that plasma protein C levels were lower in non-survivors than in survivors (6). Researches about pediatric patients with ALI/ARDS have been rarely performed though our center previously reported that decreased antithrombin III levels were associated with the risk of death in children with ALI/ARDS (12).
PT and APTT are commonly-measured values by routine laboratory tests. PT is prolonged when factor V, VII, X, fibrinogen, or prothrombin is diminished, which indicates the abnormality of the extrinsic pathway. APTT is prolonged when any of all coagulation factors except factor VII or XIII is diminished, which indicates the abnormality of the intrinsic pathway. Walsh et al. analyzed 1,923 intensive care unit admissions and reported that there was an independent association between prolonged PT and greater mortality regardless of underlying diseases (13). However, association between PT or APTT and mortality in ALI/ARDS has rarely been investigated.
We performed multivariate analysis of survival including coexistent sepsis considering that sepsis is the one of the critical variables influencing both coagulopathy and mortality. In our study, not coexistent sepsis or PRISM III score but PT and APTT were the only variables associated with both OS and FFS in the higher OI or VI groups, which represent fatal pulmonary condition. Therefore, we conclude that coagulopathy, whether resulted from ALI/ARDS itself or not, makes the outcomes of ALI/ARDS worse. However, we could not prove prolonged PT or APTT values were resulted purely from ALI/ARDS.
Reversal of abnormalities of coagulation and fibrinolysis may attenuate the progression of ALI/ARDS. A considerable number of therapeutic trials using antithrombin III, activated protein C, heparin, thrombomodulin, site-inactivated factor VIIa, and plasminogen activators have been performed for adults with sepsis (14-16) or ALI/ARDS (17-21). Administration of activated protein C is reported to have reduced mortality in severe sepsis by randomized multi-center trial (15). Replacement of antithrombin III was not proved to improve survival in sepsis (16). Evidences for benefit of these therapies targeting coagulopathy are not sufficient in ALI/ARDS.
Therapeutic effect of correction of prolonged PT or APTT by transfusion for patients with ALI/ARDS is unsure. Moreover, transfusion is known to be associated with increased risk of ALI/ARDS (22). In our study, transfusions of fresh-frozen plasma which were done in 79% of patients with or without hemorrhage did not influence outcome irrelevant to PT or APTT.
Limitations of this study include retrospective design, variable underlying diseases, and inability to use unified guidelines about mechanical ventilation, medication, and transfusion. Therapeutic options such as mechanical ventilation with low tidal volumes (23) and administration of corticosteroids (3, 24) are reported to influence mortality in ALI/ARDS. We enrolled patients from single center within 2-yr period treated by standard coherent guidelines about ventilator strategies, use of empirical antibiotics or corticosteroids, and special interventions such as renal replacement therapy which have possibilities to influence final outcome. Most of patients received mechanical ventilation with lung-protective strategy. The difference in modes of ventilation or set tidal volumes and the use of systemic corticosteroids did not influence mortality in our study. To control variables influencing coagulopathy or mortality, large-scale prospective researches should be performed.
In conclusion, PT and APTT evaluated within 24 hr after diagnosis of ALI/ARDS are associated with OS and FFS of patients with ALI/ARDS in fatal as well as less severe pulmonary condition, which supports these associations more. We suggest PT and APTT as prognostic factors in ALI/ARDS.



 XML Download
XML Download