

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is a disease characterized by airflow limitation that is not fully reversible (1). COPD is a major health problem worldwide, with a high rate of occurrence, and high costs with its management. It is the fourth leading cause of death in the world and the economic burdens associated with COPD is ever increasing (1, 2). Cigarette smoking is the most important risk factor for the development of COPD. Inhaled cigarette smoke induces lung inflammation by various inflammatory cells, such as neutrophil, macrophage, and CD4+ T cells. A variety of inflammatory mediators, such as protease, matrix metalloproteinase and tumor necrosis factor-alpha, can enhance lung parenchymal destruction, and cause airway remodeling. These inflammatory processes can result airway narrowing and airflow limitation, finally develops COPD (1, 3). However, only a small fraction of smokers develops symptomatic COPD, suggesting that genetic factors also contribute to the development of COPD (4-6).
Recently, genome-wide association (GWA) studies have identified hundreds of genetic variants influencing the risk of complex human diseases, including COPD (7-9). In addition, these GWA studies have aided our understanding of diverse molecular pathways underlying specific human diseases (10, 11). The 15q25 region that contains the nicotinic acetylcholine receptor alpha subunit 5 and 3 (CHRNA5 and CHRNA3) genes was initially identified as a lung cancer susceptibility locus through GWA studies conducted in Caucasian populations (12, 13). Subsequently, this 15q25 region has been reported to be also associated with risk of COPD in GWA studies (7, 14). However, the single nucleotide polymorphisms (SNPs), rs8034191 and rs1051730, identified in previous GWA studies for lung cancer and COPD in Caucasians (7-14), are extremely rare in Asians, according to HapMap data. Consistent with HapMap data, Wu et al. (15) reported that these two SNPs are very rare (minor allele frequencies < 0.05) in Chinese populations. Notably, they reported that among the SNPs in the CHRNA5-CHRNA3 locus, the rs6495309C > T in the promoter of the CHRNA3 gene affects the binding ability of the transcriptional factor, Oct-1, resulting in alteration of CHRNA3 expression, thereby influencing lung cancer risk (15). This finding suggests that the rs6495309C > T of CHRNA3 may be associated with the risk of COPD in Asian populations. Therefore, to verify the role of the rs6495309C > T of CHRNA3 on the risk of COPD, we have carried out a case-control study in a Korean population.
MATERIALS AND METHODS
Study population
The patient group (n = 406) consisted of male patients who visited the respiratory center in Kyungpook National University Hospital (Daegu, Korea) between July 2006 and December 2008. Diagnosis of COPD was established by the NHLBI/WHO Global Initiative for COPD (GOLD) (1). The criteria for COPD were as follows: chronic respiratory symptoms and signs such as cough and dyspnea; post-bronchodilator forced expiratory volume at one second (FEV1) < 80% of the predicted value, FEV1/forced vital capacity (FVC) < 70% and FEV1 reversibility after inhaling 200 µg salbutamol < 12% of the pre-bronchodilator FEV1. The severity of COPD was classified by the guidelines of GOLD in terms of the percentage predicted FEV1: mild (> 80%), moderate (50%-80%), severe (30%-50%) or very severe (< 30%). Control subjects (n = 394) were selected from a pool of healthy men who visited the general health check-up center. The enrollment criteria for the control subjects were as follows: male, age > 45 yr, current or former smoker, no known disease and no history of any disease, and no airflow limitation. All of the cases and controls were ethnic Koreans that resided in Daegu City, or in the surrounding regions. A trained interviewer completed detailed questionnaires for each patient and each control subject.
Genotyping
Genotypes of the rs6495309C > T was determined by melting-curve analysis using fluorescence labeled hybridization probes (LightCycler, Roche Diagnostic, Mannheim, Germany). A genotype success rate of greater than 99% was achieved using the LightCycler. Samples that could not be scored by the LightCycler were re-genotyped by direct sequencing using an ABI PRISM 3700 genetic analyzer (Applied Biosystems, Foster City, CA, USA). All genotyping analyses were performed "blind" with respect to the case/control status to ensure quality control. Approximately 10% of the samples were randomly selected to be genotyped again by a different investigator, and the results were 100% concordant with the original analysis.
Statistical analysis
The cases and controls were compared using the Student's t-test for continuous variables, and a chi-squared test for categorical variables. Deviations of genotype frequencies among controls from those expected under Hardy-Weinberg equilibrium were assessed by chi-squared test (1° of freedom). Unconditional logistic regression analyses were used to calculate the odds ratio (OR) and 95% confidence interval (CI), with adjustment for possible confounders (age, and pack-years of smoking used as continuous variables). In addition to the overall association analysis, we performed a stratified analysis according to age, smoking status, and severity of COPD to explore the association between genotypes and the risk of COPD in each stratum. A homogeneity test was performed in order to compare the difference between the genotype-related ORs of the different groups. All analyses were performed using Statistical Analysis System for Windows, version 9.1 (SAS Institute, Cary, NC, USA).
RESULTS
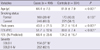
The baseline characteristics of the study population are shown in Table 1. There was no significant difference in the smoking status between cases and controls. Age and pack-years of smoking were significantly higher in cases than in controls (64.4 ± 7.5 vs 61.9 ± 7.9 yr, P < 0.001; and 43.8 ± 21.5 vs 31.7 ± 16.4 pack-yr of smoking, P < 0.001, respectively). These differences were controlled in the later multivariate analyses. The FEV1 and the FEV1/FVC ratio were significantly lower in the COPD group than in the control group (P < 0.001, both).
Table 2 shows the genotype distribution of rs6495309C > T among the cases and controls. The genotype distribution of the rs6495309C > T among the controls was in Hardy-Weinberg equilibrium. The frequency of the variant T allele among the controls was 0.494, which was comparable with that (0.482) of healthy Chineses (15). The distribution of the rs6495309C > T genotypes was significantly different between the cases and controls (CC, CT, and TT genotypes; 34.5%, 48.8%, and 16.7%, respectively vs 26.6%, 48.0%, and 25.4%, respectively; P = 0.004), with the frequency of the variant T allele being significantly lower in the cases than in the controls (0.411 vs 0.494, P = 0.001). The risk of COPD decreased as the number of T alleles increased (Ptrend = 0.002), and the TT genotype was associated with a significantly decreased risk of COPD when compared to the CC genotype (adjusted OR, 0.50; 95% CI, 0.33-0.76; P = 0.001). Individuals with the rs6495309 CT or TT genotype had a 31% (95% CI, 0.50-0.95; P = 0.023) decreased risk of COPD when compared to those with the rs6495309 CC genotype.
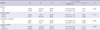
The association between the rs6495309C > T genotypes and the risk of COPD was further investigated, after stratification according to age, smoking status, and severity of COPD (Table 3). The effects of the rs6495309C > T genotype on the risk of COPD did not differ significantly between younger- and older-individuals, and former- and current-smokers (P value of test for homogeneity [PH], both, > 0.05 in all comparisons). When stratified by the median pack-years of smoking, the effect of the rs6495309C > T genotype on the risk of COPD was more evident in lighter-smokers than in heavier-smokers under dominant model for the variant T allele (PH = 0.030). When COPD cases were categorized by disease severity, the rs6495309 CT, or TT genotype was associated with a significantly decreased risk of moderate to very severe COPD (GOLD II-IV; adjusted OR, 0.56; 95% CI, 0.39-0.80; P = 0.001), whereas there was no significant association between the rs6495309C > T genotypes and the risk of mild COPD (GOLD I; adjusted OR, 1.07; 95% CI, 0.69-1.65; PH = 0.024).
DISCUSSION
In this study we determined the association between the rs6495309C > T polymorphism on the 15q25 region and the risk of COPD in a Korean population. The rs6495309T allele was associated with a significant decreased risk of COPD. This finding was in agreement with results of a previous GWA study which was carried out in Caucasians (7) in which the 15q25 region was a COPD susceptibility locus, thus providing strong evidence that the 15q25 region may play an important role in the development of COPD. This study is the first report of an association between the CHRAN3 rs6495309C > T and the risk of COPD in Asians.
Acetylcholine receptors are classified into nicotinic acetylcholine receptors (nAChRs) and muscarinic receptors, and nAChRs are historically classified as neuronal- or muscle-type based on their initial site of identification and composite subunits (16). Cholinergic parasympathetic activity in the airways induces tracheobronchial smooth muscle contraction and mucous secretion (17, 18). However, there is increasing evidence that non-neuronal cholinergic systems that are found in non-neuronal cells, such as airway inflammatory cells, modulate inflammation of the lung, and thus, contribute to the development of COPD (19). It has been shown that bronchial epithelial cells, and airway fibroblasts and inflammatory cells express nAChRs (20). Nicotine and nicotine-derived nitrosamines in cigarette smoke triggers the nAChRs of inflammatory cells of the lung to release protease and oxidants that are associated with the pathogenesis of COPD (19-21). In addition, it has been demonstrated that the rs6495309T allele significantly reduces promoter activity, which in turn diminishes CHRNA3 expression (15). Therefore, it is plausible that subjects with a lower production of rs6495309T allele for CHRNA3 might have a lower inflammatory response to smoking exposure, thus having a decreased susceptibility to COPD.
The association between the CHRNA3 rs6495309C > T and risk of COPD may be, in part, resulted from the fact that the SNP affects nicotinic dependence. It is known that nAChRs expressed in the key regions of the brain play an important role in controlling smoking behavior such as nicotine dependence (22-25). Several studies have reported that genetic variants of chromosome 15q25, including the CHRNA3 rs6495309C > T, are responsible for tobacco nicotine dependence (15, 25). In the present study, however, there were no significant differences in genotype and allele frequencies according to smoking status and smoking exposure levels (data not shown).
Although the rs6495309 in the promoter of the CHRNA3 gene has been reported to be a functional SNP, the association of the rs6495309 with COPD may be due to linkage disequilibrium (LD) with other functional variant(s) rather than a direct effect of the rs6495309. In order to identify the variant(s) that may be in strong LD with the rs6495309 that could be actually responsible for the alteration in COPD risk, we screened and estimated the LDs of all the potentially functional SNPs (with a minor allele frequency ≥ 0.05 in Asians) around the CHRNA5/CHRNA3 locus including the rs6495309 using the NIEHS database (http://manticore.niehs.nih.gov). As shown in Fig. 1, four SNPs (rs578776, rs472054, rs660652 and rs615470) were captured. However, none of these four SNPs were in strong LD with the rs6495309 based on HapMap JPT data of the public database (http://www.ncbi.nlm.nih.gov/SNP). This finding suggests that the association observed in the present study may be due to direct effect of the rs6495309. However, because the four potentially functional SNPs captured from the database may also affect the risk of COPD, future studies of these four SNPs are also needed to further understand the role of genetic variants in the CHRNA5/CHRNA3 locus in determining the risk of COPD.
In conclusion, this case-control study demonstrates a significant association of the CHRNA3 rs6495309C > T on chromosome 15q25 with the risk of COPD. Because this is the first case-control study investigating the association of the CHRNA3 rs6495309C > T with the risk of COPD in Asian populations, additional studies are required to confirm our findings.


 XML Download
XML Download