

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Diabetes mellitus (DM) is one of the most major risk factors for cardiovascular diseases, primarily as the result of adverse changes in arteries. A key change to arteries with DM that contributes to increased risk of cardiovascular diseases is the development of vascular endothelial dysfunction (1, 2), as indicated by reductions in endothelium-dependent dilation. Identifying the factors related to impaired endothelium-dependent dilation with DM is an important clinical goal because it may lead to effective strategies to prevent and/or treat DM-associated endothelial dysfunction. Ultrasound measurement of flow-mediated vasodilatation (FMD) is the most widely used non-invasive vascular test to evaluate endothelial function (3, 4).
Endothelial function is deteriorated by the attenuation of nitric oxide (NO) production (5, 6) and increased NO inactivation (7) in patients with DM. On the other hand, the impaired endothelial function improves after drug therapy or the correction of lifestyle habits. Therefore, the FMD is a useful parameter to evaluate the vascular function after treatment (8-11).
Inhibiton of dipeptidyl peptidase-4 (DPP-4) is a new mechanism for the treatment of DM that leads to increasing the action of incretins, which are gastrointestinal hormones. Glucagon-like peptide 1 (GLP-1), an incretin family member (12, 13), has been reported to promote insulin secretion in a glucose-dependent manner (14), and to inhibit glucagon secretion (15). GLP-1 improves the postprandial endothelial dysfunction (16) and left ventricular systolic function (17), and has vasodilator effects that are endothelium-dependent (18).
The clinical benefits of DPP-4 inhibitors on vascular function have not been evaluated. Therefore, the aim of this study was to measure the FMD before and after the administration of sitagliptin (a representative DPP-4 inhibitor) in patients with type 2 DM who were complicated with endothelial dysfunction, and to evaluate the impact on their endothelial function. In addition, this study compared the plasma adiponectin and asymmetric dimethylarginine (ADMA) levels, as biochemical markers that reflect the endothelial dysfunction, before and after drug administration.
MATERIALS AND METHODS
Study population
This study enrolled 40 consecutive subjects > 20 yr of age with type 2 DM and with inadequate glucose control (defined as 6.5% ≤ Hemoglobin A1c [HbA1c] < 10%) even after dietary and exercise therapies for ≥ 8 weeks. The excluded subjects were if they had type 1 DM, were taking pioglitazone (which affects the endothelial function) (19), were insulin dependent, had known impairment of renal function (estimated glomerular filtration rate [eGFR] ≤ 60 mL/min/1.73 m2), had persistent elevations of their serum transaminases, or had DM that was uncontrollable (HbA1C > 10%) by oral medicine.
Study design
This study was an open-labeled prospective observational single arm trial. The patients were treated with 50 mg sitagliptin once daily for glycemic control, and were maintained on the same dose throughout the study period (12 weeks). All patients were instructed to continue diet and exercise therapy during the study. Clinical assessments, blood sampling, and evaluations of the endothelial function, carotid intima media thickness (IMT), and brachial ankle pulse wave velocity (ba-PWV) were performed in all patients both before and at 12 weeks after treatment.
Evaluation of the effectiveness of sitagliptin
The primary endpoint was improvement of the FMD at 12 weeks. Secondary endpoints were changes in the baseline fasting blood glucose, HbA1c, immunoreactive insulin (IRI), homeostasis model assessment (HOMA) index, β-cell function, mean IMT, mean ba-PWV, adiponectin, and ADMA. In addition, the correlation of the FMD with each of those measures was evaluated.
Blood sampling and measurements
Blood samples were obtained from the antecubital vein after an overnight fast for at least 12 hr. The HbA1c levels were measured by latex agglutination, and the plasma glucose levels were determined by the glucose oxidase method. The serum IRI and lipids levels were measured by an immunoradiometic assay and enzymatic methods, respectively. The HOMA index value was calculated using the formula: (fasting blood glucose [mM] × fasting insulin [mU/L]/22.5). The β-Cell function was assessed using the formula: (20 × fasting insulin [mU/L]/[fasting glucose [mM]-3.5]) (20). The plasma adiponectin and ADMA levels were measured by latex agglutination and high-performance liquid chromatography (HPLC), respectively (SRL, Inc, Tokyo, Japan).
Flow-mediated dilatation
The patients' endothelial function was evaluated by means of the FMD, according to previously published guidelines (21). The subjects could not smoke, eat, or drink anything containing caffeine for 12 hr before the FMD measurement. The FMD was measured between 9 and 10 a.m. before patients had taken any medications.
The subjects were allowed to rest in the supine position at least 15 min before the examination, then the FMD was assessed in each right arm in a quiet, temperature-controlled (25℃) room by using a high-resolution ultrasound device (UNEXEF 18G, UNEX Corporation, Nagoya, Japan). A view of a 5 cm transverse section of the brachial artery was recorded for periods of 30 sec at baseline and during peak reactive hyperemia (after deflation of the blood pressure cuff previously inflated to 50 mmHg above the systolic blood pressure around the forearm for 5 min). The FMD was calculated as the percentage change in the diameter from the baseline value before cuff release to the peak value after cuff release. The endothelium-independent vasodilation was determined by measuring the arterial diameter in response to sublingual administration of 0.5 mg nitroglycerine after resting for at least 15 min. The nitroglycerin-mediated dilation (NMD) was calculated as the increase in the diameter 5 min after administrating nitroglycerine as a percentage of the baseline diameter.
Carotid intima media thickness
The IMT was measured using the LOGIQ E9 instrument (General Electric Co., Ltd, Tokyo, Japan) with a 7 MHz linear array transducer. The patients were examined in the supine position with their neck extended and the probe was placed parallel to the common carotid artery (CCA). B-mode scans were obtained with electronic calipers. Three points each in the right and left CCA were measured and averaged.
Brachial ankle pulse wave velocity
The ba-PWV was measured using a volume-plethysmographic apparatus (from PWV/ABI; Colin Co., Komaki, Japan) with the patient in a supine position after 5 min of rest. This device simultaneously records the phonocardiogram, electrocardiogram, and volume pulse form and arterial blood pressure at both the left and right brachial and ankles. The ba-PWV was calculated by time-phase analysis between the right brachial and volume waveforms at both ankles. The distance between the right brachium and ankle was estimated based on the body height. The mean ba-PWV was used in the analyses because the right and left ba-PWV are significantly correlated (22).
Relevant factors
The pulse rate and blood pressures (BP) were measured at rest, simultaneously with the measurement of the ba-PWV. The patients' height and weight were measured at the time of ba-PWV measurement, and the body mass index (BMI: kg/m2) was calculated as an index of obesity. The value for HbA1c (%) was estimated as an NGSP equivalent value (%) calculated by the formula HbA1c (%) = HbA1c (JDS) (%) + 0.4%, considering the relational expression of HbA1c (JDS) (%) measured by the previous Japanese standard substance and measurement methods and HbA1c (NGSP). Hypertension was defined as blood pressures ≥ 140/90 mmHg or the current use of antihypertensive agents. Dyslipidemia was defined as low-density lipoprotein-cholesterol (LDL-C) ≥ 3.62 mM or the current use of lipid-lowering agents. Chronic kidney disease was defined as patients with an eGFR ≤ 60 mL/min/1.73 m2. The eGFR was estimated using the simplified prediction equation derived from the modification of diet in renal disease study (23).
Statistical analysis
The SPSS ver. 16.0 software program was used for the statistical analysis. Differences between before and after administration were analyzed by employing one-way ANOVA, following unpaired t-test. Quality-assurance methods included previously described written protocols and measurement variability assessments (21). Reproducibility results compared the 3 sonographers' measurements of 20 studies separated by 1 yr. The coefficient of variation (CV) of inter-observer variability in FMD was 7.15%, which is the reasonable data to assess FMD value using edge-detection software compared with the analysis by hand (24). Also, CV of the intra-observer difference in FMD was 5.81%. And CV of inter-measurement variability in FMD was 2.95%. A Pearson's correlation analysis was carried out to determine the correlation of the changes of the FMD with variables such as age, male, smoking, those of fasting blood glucose, HbA1c, IMT, ba-PWV, adiponectin, and ADMA. A multivariate linear regression analysis was carried out using the changes of the FMD as the dependent variables and age, male, smoking, those of fasting blood glucose, HbA1c, IMT, ba-PWV, adiponectin, and ADMA as independent variables. A P value < 0.05 was considered to be significant.
RESULTS
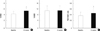
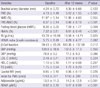
A total of 42 subjects were initially enrolled in this study. Two participants withdrew because of nausea and upper abdominal discomfort during the second week of sitagliptin treatment. The mean age of the remaining 40 participants was 68.9 ± 10.4 yr. The mean duration of diabetes was 4.4 ± 2.0 yr with an HbA1c of 7.3% ± 0.8%. The baseline clinical characteristics of the subjects are summarized in Table 1. Some subjects were on oral antidiabetic agents, including sulfonylureas (n = 13), α-glucosidase inhibitors (n = 10), biguanides (n = 13), and the other 17 were not taking any medicine. The changes in the various biochemical parameters after the 12 weeks treatment are shown in Table 2. The %FMD and FMD/NMD ratio were significantly (P < 0.001) increased, whereas the %NMD did not change (Fig. 1). The HbA1c, fasting blood glucose and ADMA levels were significantly (P < 0.001) decreased by the treatment. In addition, the plasma adiponectin levels were significantly (P < 0.001) increased. On the other hand, the fasting IRI, HOMA index of insulin resistance, carotid IMT and ba-PWV did not change.
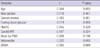
Table 3 shows the univariate correlations between the changes of the FMD and those of various parameters after the 12-week treatment with sitagliptin. The changes in the FMD were significantly (P < 0.05) correlated with those of the plasma adiponectin level (r=0.329; Fig. 2). The changes in the FMD showed no significant correlations with those of fasting blood glucose, HbA1c, ADMA, mean IMT or mean ba-PWV.
A multivariate linear regression analysis was done using the changes of the FMD as dependent variables; the results are listed in Table 4. The changes of the FMD showed a positive association with those of the plasma adiponectin (P = 0.043).
DISCUSSION
The current findings were that %FMD was increased, NMD did not change, HbA1c and ADMA levels were decreased (P < 0.001), plasma adiponectin levels were increased (P < 0.001) after 12 weeks of treatment. A multivariate linear regression analysis showed that the changes of the FMD had a positive association with those of the changes of the plasma adiponectin. The present study revealed that the sitagliptin reversed endothelial dysfunction (FMD/NMD ratio that indicated the true endothelium function) in type 2 DM patients. This implied that the treatment of type 2 DM patients selectively improved the endothelial function without affecting the vascular smooth muscle function because other vascular factor such as mean IMT, and mean ba-PWV were not changed.
Many reports regarding the relationship between DPP-4 and endothelial function have suggested the potential physiological mechanisms underlying this activity. First, DPP-4 inhibition by sitagliptin may be expected to increase the circulating levels of GLP-1. GLP-1 based therapy improves the postprandial endothelial dysfunction (16, 25, 26). Furthermore, animal studies demonstrate that GLP receptors are located in myocardial, vascular endothelial, and smooth muscle cells, and GLP-1 induces improvements in the cardiac function, as well providing cardioprotective effects, through the elevation of cAMP levels (17, 18). These protective effects are also likely mediated via cAMP-dependent protein kinase A (PKA) activation by sitagliptin (27). Therefore, sitagliptin may increase the cAMP levels, thus leading to a significant regression of arteriosclerotic lesions.
Second, there was a positive correlation between the changes of the FMD and those of the plasma adiponectin level. Adiponectin directly stimulates NO production by endothelial nitric oxide synthase (eNOS). Therefore, the increased adiponectin level likely exerts anti-atherosclerotic effects and improves the insulin resistance (19). The plasma adiponectin level was increased after sitagliptin treatment, thus suggesting that it may have been at least partially responsible for the improved endothelial function as a result of enhanced NO production.
Furthermore, the plasma ADMA level was decreased after sitagliptin treatment in the current study. Elevated levels of ADMA inhibit NO synthesis, and therefore impair the endothelial function and promote atherosclerosis (28). A high plasma concentration of ADMA is associated with the IMT, left ventricular hypertrophy and with increased cardiovascular events, particularly in patients with diabetes. The blood ADMA levels correlate inversely with the vascular endothelial function as evaluated by the FMD (29), and vasodilator responses improve the ADMA levels (30). The current results did not show a negative correlation between the changes of FMD and those of plasma ADMA probably due to small number of subjects or to the short follow-up period. ADMA levels were significantly decreased following treatment, suggesting that it may have a potential effect on the endothelial function in production of NO, will lead to vasodilatation in long term follow-up.
No significant changes in the serum lipid profile were observed after sitagliptin treatment in this study, although an increase in HDL-C and a decrease triglycerides has been reported previously (31). In addition, sitagliptin treatment is associated with a decrease in the BP (32). The BP showed a non-significant reduction in the current study (P = 0.13). These data probably reflects the small number of subjects.
Several studies have shown that the FMD is impaired in diabetic patients (33). Improvement in the FMD by hypoglycemic agents (pioglitazone [19, 34], gliclazide [35], and glimepiride [11]) has been reported, but the impact of DPP-4 inhibitors has rarely been evaluated. Endothelial dysfunction is a marker of the very early stage of atherosclerosis, and a close relationship exists between the endothelial function in the human coronary circulation and peripheral circulation (36). The improvement of the %FMD observed after the 12 weeks of treatment with sitagliptin in the present study might lead to a decrease in cardiovascular events. In fact, the previously published meta-analyses summarizing the effects of DPP-4 inhibitors on major cardiovascular events in phase 2 and 3 studies all suggest that they lead to a lower relative risk compared with placebo or other medications (37, 38).
The limitations of the present study include that it was conducted at a single academic center. This study was done in a single arm. In addition, patients received other medications that may have affected the FMD (e.g. statins, angiotensin converting enzyme inhibitors), but their use was similar between the group at baseline, and patients were requested not to change their medications during the study. In addition, the trial was conducted for only 12 weeks. Furthermore, DPP-4 inhibitor improved endothelial function in relation to the glucose profile, such as fasting blood glucose and HbA1c. Finally, the study did not have a sufficient statistical power to detect any small changes in the HOMA index of insulin resistance due to the relatively small number of patients enrolled, and there were no patients who experienced the primary end-points.
The DPP-4 inhibitor sitagliptin improved vascular endothelial function in Type 2 DM patients. In addition, the changes of the FMD positively correlated with those of the plasma adiponectin. These observations need to be confirmed in large cardiovascular outcome studies with long-term follow up of patients.



 XML Download
XML Download