

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Chronic eosinophilic pneumonia (CEP), a rare eosinophilic lung disease of unknown etiology, is characterized by peripheral blood eosinophilia and abnormal eosinophil accumulation in the lungs (1). CEP most commonly affects middle-aged women and is accompanied by asthma in more than 50% of cases. Symptoms of CEP can be easily relieved by systemic corticosteroid therapy; however, in most cases, recurrences are frequent after the end or tapering off of systemic corticosteroids, especially in those with a prior diagnosis of asthma (2, 3).
Anti-IgE treatment reduces circulating free IgE level, down-regulates high-affinity IgE receptors (FcεRI) expression in inflammatory cells, and decreases serum and tissue eosinophil counts in many allergic diseases, including asthma, rhinitis, chronic urticaria and eosinophilic gastrointestinal disorders (4-7). However, the efficacy of anti-IgE therapy in CEP has not been studied. Here, we first report two cases of CEP that were successfully treated with anti-IgE therapy.
CASE DESCRIPTION
Case 1
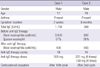
A 17-yr-old non-smoking male presented with a 2-week history of dry cough and dyspnea on exertion at August 2009. The patient had a cough and shortness of breath during running at school 9 months prior and was diagnosed with bronchial asthma. However, his asthma was not well controlled since he did not use regular maintenance therapy. During initial physical examination, coarse breathing was heard in both lower lung fields. The patient's white blood cell count was 12,100 cells/mL with 29.6% eosinophils. Ground glass opacities were found in the patient's lungs by chest computerized tomography (CT). A sputum differential count showed 97% eosinophils. The patient's total IgE level was 1,758 IU/mL and he was sensitized to birch pollen by an allergy skin prick test. Serological testing for parasites (Toxocara, Anisakis, cysticercus, Paragonimus, sparganum, and Clonorchis) produced negative results. After 14 weeks of systemic (0.5-1 mg/kg) and regular inhaled corticosteroids, the patient's serum eosinophil count was normalized (50 cells/mL). However, after tapering off of the oral corticosteroid dose, the patient's peripheral eosinophil count was increased again to 2,200 cells/mL and multiple new patchy consolidations were found by chest X-ray and CT. To reduce steroid requirement and eosinophil activation, 300 mg (4 mg/kg of body weight) of anti-IgE antibodies were administered by injection every 2 weeks. After 10 cycles of anti-IgE therapy, the patient stopped taking oral corticosteroid. The patient maintained a normal peripheral eosinophil count with no evidences of eosinophilic infiltration on radiologic findings. After 18 cycles of therapy, his asthmatic symptoms have been well controlled for more than 2 yr using only an ICS/LABA inhaler as maintenance medication. The patient's peripheral eosinophil counts remain normal with no evidence of relapse, and he continued to have normal chest X-rays (Table 1).
Case 2
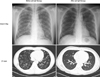
A 19-yr-old non-smoking male presented with a history of cough, sputum, dyspnea on exertion and weight loss at August 2007. This patient had been diagnosed with asthma and was treated for 8 months prior. The patient had a white blood cell count of 10,900 cells/mL with 7.2% eosinophils. A ground glass opacity was found in the patient's right middle and left lower lobes on CT; high sputum eosinophil counts were also found (56%). The patient's total IgE level was 368 IU/mL, and he was sensitized to house dust mite on skin prick test. Serological testing for parasites (Toxocara, Anisakis, cysticercus, Paragonimus, sparganum, and Clonorchis) produced negative results. After using a budesonide/formoterol inhaler and systemic oral corticosteroid, the patient's lung infiltration and peripheral eosinophil count decreased; however, when we tried to reduce the systemic steroid dose, the patient suffered recurrent respiratory symptoms with newly generated peripheral and lung eosinophilia several times over a 12-month period. To reduce the patient's systemic steroid requirement and peripheral eosinophil activation, injections of 225 mg (4 mg/kg of body weight) of anti-IgE antibodies were administered every 2 weeks. After two injections, the patient noticed significant improvement in his asthma symptoms and stopped taking systemic steroid. In total, the patient received 10 cycles of therapy. His asthmatic symptoms, peripheral eosinophil count, and radiologic finding have been well maintained using an ICS/LABA inhaler with no evidence of relapse for 15 months (Table 1, Fig. 1).
DISCUSSION
CEP was first distinguished from other associated eosinophilia syndromes in 1969 (7). The onset of the disease is usually insidious, and the symptoms appear at least a few months before diagnosis. Both cases in this article diagnosed as having asthma several months ago before the onset of CEP, and had insidious symptoms with peripheral and bronchial eosinophilia in sputum differential count and radiologic studies. We diagnosed CEP with above conditions, and treated with systemic corticosteroid in both cases. Although CEP responds well to systemic corticosteroid therapy during its initial phase, there is limited consensus concerning the long-term natural history and associated treatment regimens. In 1993, Naughton et al. (3) reported on long-term (10 yr) prognosis of patients with CEP. Seven of 9 patients who were tapered off steroids experienced clinical, hematologic, and radiologic relapses. Twenty-five percent of the patients were maintained on a regimen of low-dose steroid therapy (3). These data suggest that most of CEP patients require long-term, low-dose systemic corticosteroid therapy in order to induce symptom remission and to prevent recurrent eosinophilic infiltration into the lungs. The two cases presented in this study showed recurrent peripheral and pulmonary eosinophilia after the reduction of systemic oral steroid. Therefore, we tried anti-IgE therapy to reduce the patients' systemic steroid requirement and observed that they have maintained the remission state without relapse.
One of the most novel and striking new drugs in allergy field is anti-IgE antibody, which has the ability to control many allergic diseases, including asthma, rhinitis, eosinophilic gastrointestinal disease, and refractory urticaria (4-7). Anti-IgE therapy results in a rapid reduction of free IgE levels and the down-regulation of FcεRI on basophils, mast cells, and other inflammatory cells. Moreover, anti-IgE therapy has profound and significant reducing effects on airway and tissue eosinophilia in patients with mild allergic asthma and on allergen-induced seasonal increases in circulating and tissue eosinophils in subjects with allergic rhinitis (4, 7). Although the exact mechanism underlying the reduction in eosinophils by anti-IgE therapy remains unclear, some possible mechanisms have been suggested. Masanari et al. (9) showed that the reduction in eosinophils was more significant in those who had a low post-treatment free IgE level (< 50 ng/mL) than in those who had a relatively high post-treatment free IgE level (> 50 ng/mL) after anti-IgE injection. This suggests that a direct interaction with IgE receptors on eosinophils is a contributing factor. Noga et al. (10) found that the eosinophil apoptosis marker Annexin V was significantly elevated in patients after anti-IgE treatment. Additionally, the secretion of GM-CSF, a vital cytokine for eosinophil survival, was reduced after anti-IgE treatment compared to those taking a placebo. These results suggest that eosinophil reductions during anti-IgE therapy are caused by the induction of apoptosis through reduced GM-CSF secretion by T lymphocytes. Anti-IgE antibody therapy may give a beneficial effect for the patients with eosinophilia related conditions such as CEP.
In the present study, both patients benefited from anti-IgE therapy. Neither patient suffered from CEP-related respiratory symptom aggravation, and both stopped oral steroid use. No evidence of eosinophil activation in peripheral blood or lung tissues has been shown in follow-up studies. To date, the only treatment modality for recurrent CEP is systemic steroids. Considering the serious adverse reactions caused by long-term systemic steroid treatment, this study supports the use of anti-IgE therapy for the induction of remission in patients with CEP.
 XML Download
XML Download