

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The metabolic syndrome (MetS) is characterized by visceral adiposity, insulin resistance, dyslipidemia and increased blood pressure. It is not a single disease but a cluster of risk factors for atherosclerotic coronary artery disease (CAD) (1, 2). Consequently, the MetS has come to the fore as a major risk factor of CAD (3, 4). Isomaa et al. (5) reported that patients with the MetS had a higher incidence of CAD and increased all-cause mortality than those without it, but other researchers failed to verify these relationships (6, 7). Thus, unlike diabetes mellitus, which is a well-known established risk factor for CAD (8, 9), whether MetS has an additive impact on the development of CAD in addition to its individual components (e.g., hypertension, diabetes) is controversial (10). Conversely, it has been reported that the summation of the constituents of the MetS, the MetS score, is related to a higher incidence of CAD (11, 12).
The authors reported previously that epicardial fat measured by echocardiodraphy is related to the extent of coronary atherosclerosis in patients undergoing their first coronary angiography (13). From the data, we evaluated the relationship between the MetS score and CAD severity as assessed by angiography according to the presence of diabetes. Whether the MetS predicts angiographic CAD beyond well-established risk factors for CAD was also investigated.
MATERIALS AND METHODS
Study population
We collected clinical, biochemical, and angiographic information for 527 consecutive patients aged > 18 yr (267 males; mean age, 58.4 ± 10.8 yr) who underwent their first coronary angiography due to chest pain between January 2005 and October 2005 at Ajou University Medical Center. The medical records of all patients were reviewed. Patients were excluded if they had a history of percutaneous coronary intervention, coronary artery bypass graft, acute ST-segment elevation myocardial infarction, active inflammation, heart failure, chronic kidney disease, severe liver disease or cancer.
Anthropometric measurements such as the body mass index (BMI), waist circumference and hip circumference were collected. Plasma lipid profiles and levels of C-reactive protein (CRP), fibrinogen, uric acid and cardiac enzymes were measured. The homeostasis model assessment of insulin resistance (HOMA-IR) was calculated in non-diabetic patients using fasting plasma insulin concentrations and glucose concentrations as previously described (14). Patients with more than three of five criteria based on the updated guidelines issued by the Adult Treatment Panel (ATP III) of the National Cholesterol Education Program were considered to have the MetS. Central obesity was considered to be present if the waist circumference was > 90 cm in men and > 80 cm in women; these are the threshold values for Asian populations (15, 16). The MetS score was defined as the number of MetS components present.
Angiographic studies
On quantitative analyses of coronary angiograms (Quantcor QCA, version 4.0; Pie Medical Imaging, Maastricht, The Netherlands), the presence of stenosis ≥ 50% in diameter of major epicardial vessels was defined as CAD. The extent of CAD was quantified using the number of vessels with ≥ 50% stenosis and a coronary atherosclerosis score as follows (17). The coronary artery tree was divided into nine segments: left main coronary artery; proximal, mid-, and distal left anterior descending artery; proximal circumflex artery (including the first obtuse marginal branch); circumflex artery distal to the first marginal branch; proximal and mid-right coronary artery; posterior descending artery. Each of these segments was scored from 0 to 3 depending on the most severe stenosis according the following system: 0 = normal; 1 = stenosis of 1%-49%; 2 = stenosis of 50%-99%; and 3 = total occlusion. A coronary atherosclerosis score was generated as the sum of the scores in all segments.
Statistical analyses
SPSS version 17.0 (SPSS Incorporated, Chicago, IL, USA) was used for statistical analyses. Continuous variables were expressed as mean and standard deviation, and categorical variables as number and percentage. Comparisons of differences in anthropometric and biochemical values, and frequencies of CAD risk factors, CAD, and multi-vessel disease according to the presence of the MetS were undertaken using the Student's t-test and chi-squared test. Correlations of the MetS score with various clinical and biochemical parameters were examined by the Spearman's rank correlation analysis. Using one-way analysis of variance, the relationship between the MetS score and the extent of coronary atherosclerosis was explored in diabetic and non-diabetic subjects. A set of well-recognized risk factors for CAD (age; history of hyperlipidemia, hypertension, and diabetes; family history of early atherosclerotic CAD; current smoking; and elevated levels of CRP ≥ 1 mg/L) were included in a logistic regression model of angiographic CAD (1, 17). The presence of the MetS was then added to this model to determine if there was an additional predictive value. Statistical significance was considered at P < 0.05.
RESULTS
Baseline characteristics
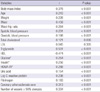
A summary of anthropometric, biochemical, and clinical characteristics according to the presence of the MetS is shown in Table 1. A total of 327 (62%) patients had the MetS, and 447 (85%) patients had more than two components of the MetS. The mean MetS score was 2.8 ± 1.3. Among patients with the MetS, an elevated fasting glucose level (85.6%) was the most frequent component followed by high blood pressure (85.3%), waist circumference (77.7%), high-density lipoprotein (HDL) cholesterol (61.2%) and triglyceride (TG; 56.3%). The HOMA-IR of non-diabetic patients (n = 402) was elevated in those with the MetS. The level of CRP was higher in those with the MetS. No difference was found in the level of low-density lipoprotein (LDL) cholesterol between the two groups.
Relationship between the MetS score and anthropometric, biochemical and angiographical variables
Spearman's rank correlation analysis showed that the MetS score was positively associated with age, weight, waist circumference, blood pressure, the HOMA-IR, as well as levels of total cholesterol (TC), TG, glucose, insulin, uric acid, CRP and fibrinogen, and negatively associated with the HDL-cholesterol level (Table 2). There was no association between the MetS score and LDL-cholesterol level. The degree of correlation between the MetS score and TG level was highest, followed by that with HDL cholesterol, waist circumference, BMI, and HOMA-IR.
Relationship between the MetS score and severity of coronary atherosclerosis according to the presence of diabetes
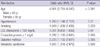
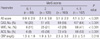
A total of 195 of 260 CAD patients (75%) had the MetS. The frequency of CAD and multi-vessel disease was higher in patients with the MetS compared with those without it (60% vs 32%, P < 0.001; 34% vs 16%, P < 0.001, respectively). Participants with at least two components of the MetS who did not meet the criteria for the definition of the MetS had a higher frequency of angiographic CAD (55% vs 16%, P < 0.001) and multi-vessel disease (30% vs 8%, P < 0.001) and a greater atherosclerosis score (3.3 ± 3.4 vs 1.0 ± 2.0, P < 0.001) in comparison with those with less than one MetS component. Patients with the MetS and diabetes had the highest coronary atherosclerosis score, followed by diabetic patients without the MetS, the MetS without diabetes, and patients with neither diabetes nor the MetS (4.5 ± 3.3, 3.8 ± 4.3, 3.1 ± 3.4, and 1.6 ± 2.8, respectively) (Fig. 1). On multiple logistic regression analysis, the MetS was independently associated with angiographic CAD (Table 3). In the overall population, the frequency of CAD, multi-vessel disease, coronary atherosclerosis score, and CRP level increased with MetS score (Table 4). These relationships persisted in non-diabetic individuals, whereas no relationship was found between the MetS score and coronary angiographic atherosclerosis in diabetic patients (Table 5).
Relationship between the MetS and disease activity
As the MetS score increased, so did the frequency of acute coronary syndromes and CRP level (Table 4). Patients presenting with ACS (n = 212) had higher MetS scores compared with those with atypical chest pain or stable angina (3.3 ± 1.0 vs 2.6 ± 1.4, P < 0.001).
DISCUSSION
The aim of the present study was to investigate the relationship between the MetS score and CAD severity according to angiography and to determine if it differed based on the presence of diabetes. The MetS score influenced the severity of coronary atherosclerosis in non-diabetic patients, but there was no relationship between the MetS score and coronary atherosclerosis in diabetic subjects.
The MetS is determined by the presence of ≥ 3 quantitatively identified markers. It has been regarded to be an important risk factor for CAD and a predictor for cardiovascular events (1-5). Some authors have raised the question of whether it has additive prognostic value for CAD in tandem with its individual components. It was suggested that attempts to define a criteria of the MetS that simultaneously predicts for CAD and diabetes are unhelpful because the MetS had weak or no association with cardiovascular risk (6, 10, 18, 19). Those findings indicated that the MetS is a marker of CAD risk, but not above and beyond the risk associated with its individual components. In our cohort, elevated fasting glucose level and high blood pressure were the most frequently encountered factors in patients with the MetS. Our findings coincided with studies in which high blood pressure and a high fasting blood glucose level were strongly related to cardiovascular mortality among individual MetS components (10). The MetS remained an independently associated factor for angiographic CAD on multiple logistic regression analysis. Thus, glycemic level and high blood pressure are the most critical components of the MetS for the development of CAD, and the MetS might have an additive effect on the severity of coronary atherosclerosis beyond that of its individual components.
We also sought to investigate the usefulness of counting individual factors of the MetS for prediction of CAD. Increasing MetS score was significantly related to increasing coronary atherosclerosis score, consistent with the results of other studies (11, 12). Patients with more than two components of the MetS not fulfilling the criteria for the diagnosis of the MetS had a higher atherosclerosis score and more multi-vessel disease than subjects with one or fewer than one component of the MetS. Counting the components of the MetS appears to be more valuable for risk stratification for CAD than dichotomously diagnosing the MetS if there are more than three arbitrary components. To verify the relationship between the MetS score and coronary atherosclerosis in diabetes, we divided the study cohort into two groups based on the presence of diabetes. In non-diabetic subjects (n = 402), the relationship between the MetS score and the severity of coronary atherosclerosis persisted, whereas there was no such association in diabetic subjects (n = 125). These findings might be due to attenuation of the impact of the MetS on the development of CAD by the presence of diabetes (a well-recognized strong risk factor for CAD). Similarly, Zornitzki et al. (7) showed that only diabetes (and not the MetS) predicted the severity and extent of CAD in women. Therefore, the MetS score does not seem to be useful for prediction of the extent of CAD in the presence of diabetes.
It has been reported that the MetS imparts an increased risk of cardiovascular events after the first myocardial infarction (20). Lee et al. (21) showed that the MetS was an important predictor for in-hospital death in patients with ST-elevation myocardial infarction. CRP as a marker of vascular inflammation may have a role in increasing CAD activity as well as in promoting coronary atherosclerosis (17, 22, 23). Ridker et al. (24) demonstrated that the MetS score was well correlated with the CRP level, which is consistent with our results. Patients with acute coronary syndrome had a higher MetS score than those with atypical chest pain or stable angina. These findings suggest that accumulating individual components of the MetS may increase vascular inflammation, leading to heightened CAD activity. Thus, the MetS score and CRP level are closely related. The MetS score and CRP level could help us better predict future cardiovascular events in patients with established CAD as well as in those without CAD.
The present study had several limitations. First, the study group contained only Korean patients undergoing their first coronary angiography due to chest pain. Second, the design of our study was cross-sectional. Third, the coronary atherosclerosis score does not represent the actual atheroma volume or plaque burden; it is a crude method for estimating CAD severity. However, coronary angiography is the most widely used technique for assessing coronary anatomy, and this score was validated in a study that compared CRP level with the extent of CAD (17).
In conclusion, the MetS score can be readily obtained and calculated in most clinical situations. Although the association between the MetS score and angiographic CAD severity may be obscured by the presence of diabetes, the MetS score is related to the severity of coronary atherosclerosis in non-diabetic patients. Calculating the MetS score might provide additive information for predicting the extent of CAD in non-diabetic patient with angina.



 XML Download
XML Download