

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Abdominal obesity is one of the most important risk factors for acute myocardial infarction among adults, presenting an attributable risk of 20.1% (1). This concern extends to adolescents since central fat has been shown to be associated with an increased risk of cardiovascular diseases during this phase of life (2, 3).
Despite the availability of more sophisticated methods for the evaluation of abdominal fat, waist circumference (WC) is an easy-to-use, low cost and simple measure of adiposity in epidemiological studies (4). In addition, WC is an anthropometric indicator related to abdominal fat (4) that is strongly associated with metabolic risk factors such as diabetes and dyslipidemias (2, 3).
Studies indicate that both genetic and environmental factors contribute to increased abdominal obesity, but the latter exert a greater influence and can be modified by changes in lifestyle such as adequate dietary habits and regular physical exercise (1, 5, 6). Socioeconomic and demographic factors are also associated with abdominal obesity and the identification of these characteristics may permit more effective interventions for the treatment and prevention of this condition (6).
Knowledge about factors associated with abdominal obesity in adolescents is still limited, in part, because of the lack of population-based studies and the scarcity of studies investigating different associated factors. Studies conducted in different countries have shown variations in the factors associated with abdominal obesity (2, 3, 5). In India, gender, age and nutritional status were found to be associated with excess central fat (3). In contrast, a comparison between the United States and South Korea demonstrated a relationship between metabolic factors and abdominal obesity (2). In Brazil, Fernandes et al. (5) found that family factors such as maternal and paternal nutritional status were more associated with abdominal obesity than demographic characteristics.
In view of the different factors that predict abdominal obesity, the objective of the present study was to investigate the effects of socioeconomic, demographic and lifestyle factors on abdominal obesity in adolescent students from a Brazilian state capital.
MATERIALS AND METHODS
Population and sample selection
An analytical and descriptive cross-sectional study was conducted in the second semester of 2007 in the city of Florianópolis, Santa Catarina, Brazil.
The adolescents were selected from state public schools of the city of Florianópolis, Santa Catarina, Brazil, and sampling was performed in two phases: stratification according to geographic region and cluster sampling of classes. In the first phase, the city was divided into five geographic regions: center, continent, east, north, and south. The largest schools in each region were selected from the list of schools (Coordination of School Census and Statistics, Ministry of Education, Sciences and Technology of the State of Santa Catarina), and classes sufficient to reach representativeness of the geographic area were selected by drawing lots in each school. In the second phase, all adolescents who were present in the classroom on the day of data collection were invited to participate in the study.
Various sample sizes were calculated since this study was part of a larger research project investigating different health outcomes. The sample chosen for the present study was that selected for the analysis of the prevalence of abdominal obesity. A prevalence of the outcome of 15% (5) was adopted, with a tolerable error of 4%, a confidence interval of 95% and a design effect of 1.5, adding 20% for possible losses. Thus, 538 students need to be evaluated. In view of the sampling process that involved all subjects of the clusters, 892 adolescents participated in the sample.
Eligibility criteria included enrollment in state schools, presence in the classroom on the day of data collection, and age ≤ 19 yr. This cut-off was chosen based on the criteria of the World Health Organization (7) defining the beginning and end of adolescence (10 to 19 yr). Exclusion criteria were age > 19 yr, pregnancy, lack of informed consent provided by the responsible person (students < 18 yr) or the participant himself (18 yr or older), refusal to participate in the study, and an incomplete questionnaire.
Data collection
The field study was conducted by a team of four physical education teachers. The examiners were trained in all necessary procedures in order to standardize the data collection. Each examiner was responsible for the collection of one measurement and/or test to prevent interobserver variability and to increase the reliability of the data. During the field study, the students were informed about the evaluations at least 3 days prior to the assessment. The tests were performed preferentially during the physical education classes and the free informed consent form and detailed information about the procedures were provided to the students on that occasion.
WC was measured in duplicate using a standard method (8). According to the protocol, WC was measured at the minimum circumference between the iliac crest and the rib cage at the end of a normal expiration. The critical values proposed by Taylor et al. (4) were used to define abdominal obesity. These values were used because WC identified a high proportion of children and adolescents with high trunk fat mass (z score ≥ 1) as measured by dual energy radiography absorptiometry (DXA) (4). Moreover, the critical values presented 89% sensitivity (95% confidence interval [CI]: 77%-96%) and 94% specificity (95% CI: 91%-97%) for girls and 87% sensitivity (95% CI: 74%-95%) and 92% specificity (95% CI: 88%-95%) for boys (4).
For the assessment of nutritional status, body weight and height were measured (8) and the body mass index (BMI) was calculated. International BMI cut-off values for adults (9) were used to define "normal weight" (< 24.99 kg/m2 for age and gender) and "excess weight" (> 25 kg/m2) in adolescents.
Demographic and socioeconomic data were used as exposure variables: gender (male and female), age (continuous), school grade (10th, 11th, and 12th grade), educational level of household head (≤ 8 and > 8 complete years), and socioeconomic status. The Brazilian "ensino médio" (middle school education) corresponds to the North American High School and consists of three grades (10th, 11th, and 12th). The socioeconomic status was identified by application of the questionnaire of the Brazilian Association of Research Companies (ABEP) (10), which uses a sum of scores to divide the Brazilian population into the following five socioeconomic classes according to purchasing power, in decreasing order: A, B, C, D, and E. In the present study, a preliminary analysis of frequencies resulted in the combined classification of classes A + B, and C + D + E.
Data regarding the physical activity behavior of the adolescents were collected using the instrument proposed by Marcus et al. (11), which classifies the stages of change in physical activity behavior. On the basis of their replies, the students were classified as sedentary (pre-contemplation, contemplation and preparation stages) and active (action and maintenance stages). Data regarding the efficacy, sensitivity and specificity of this classification are reported in the literature (12).
The eating habits of the students were evaluated based on the following question: I often eat excess: 1) sugar, 2) salt, 3) animal fats, and 4) junk foods. Five reply options were given: (a) four items, (b) three items, (c) two items, (d) one item, and (e) no item. Replies to option (e) were classified as adequate eating habits, whereas the other options were classified as inadequate eating habits. This question is part of the Fantastic Lifestyle Questionnaire (8) that was translated and validated for the Brazilian population (13).
Aerobic fitness was measured and classified according to the criteria of the Canadian Physical Activity, Fitness and Lifestyle Appraisal (8). A step ergometer was used for the bench step test, with the subject stepping on and off at a rhythm established by the test protocol. At the end of the test, an aerobic fitness score is generated as follows: aerobic fitness score = 10 × [17.2 + (1.29 × O2 consumption)-(0.09×body weight in kg)-(0.18 × age in years). This score is then used to classify each component into five categories related to health benefits: (a) requires improvement, (b) regular, (c) good, (d) very good, and (e) excellent. In the present study, physical fitness was classified as adequate (categories c, d and e) and inadequate (categories a and b).
Statistical analysis
Descriptive statistic parameters (mean, standard deviation, and absolute and relative frequency) were used. The Student t-test for independent samples was used for the comparison of BMI and WC between genders.
A hierarchical multivariate model was used for the analysis of abdominal obesity (Fig. 1). In this model, the decision of inclusion of the variables in the analysis followed the relationship hierarchy between variables. For the evaluation of abdominal obesity, the variables that belong to Block I were the first to be introduced into the model since they act on the outcome but are not determined by variables close to the outcome. The first block (Block I) included demographic and socioeconomic variables. Behavioral variables that are determined by variables of the upper (distal) block were included in Block II. Block III included the aerobic fitness variable which was also determined by behavioral factors and, at the same time, influenced BMI, reflecting on nutritional status present in Block IV that was proximal to the outcome, i.e., the occurrence of abdominal obesity. Variables with at least one category presenting a P value < 0.20 in the Wald test were introduced into and/or kept in the multivariate model and were considered to be a potential confounding factor for the proximal block. Binary logistic regression was used since the outcome variable presented a low prevalence in the sample. Statistical analysis was performed with the SPSS program, version 15.0, and odds ratios and the respective 95% confidence interval were calculated.
Ethics statement
The study was approved by the institutional review board and ethics committee on research involving humans of Universidade Federal de Santa Catarina (protocol 372/2006). Written informed consent was obtained from each parent or guardian (for adolescents < 18 yr) or from the adolescents themselves (for those ≥ 18 yr).
RESULTS
In the sample selected, 16.0% of the students refused to participate in the anthropometric assessment and fitness test, 8.4% were excluded because the socioeconomic and demographic questionnaire was incomplete, and 2.0% because they were outside the age range established. Thus, the final sample consisted of 656 high school students with a mean age of 16.1 yr (standard deviation = 1.1).
As shown in Table 1, most adolescents were females (64.5%) and from a medium to high socioeconomic class (70%), the household head had more than 8 yr of schooling (68.4%), and most students were enrolled in the 11th grade (39.3%), sedentary (54.4%), presented inadequate eating habits (93.1%), good aerobic fitness (68.6%), and a normal nutritional status (87.2%).
The prevalence of abdominal obesity in the sample was 6.6% (95% CI: 4.6-8.4). The highest prevalence of abdominal obesity was observed among adolescents enrolled in the 10th grade (10.6%) and among adolescents presenting low aerobic fitness (15.5%) and excess weight (48.8%). The prevalence of abdominal obesity was similar for the other variables (Table 1).
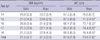
As can be seen in Table 2, the BMI was similar in girls (21.0 ± 3.7 kg/m2) and boys (21.3 ± 3.5 kg/m2) at all ages (P > 0.05). Boys presented a greater WC (73.0 ± 7.6 cm) than girls (67.9 ± 7.8 cm) at most ages (P < 0.05).
Table 3 shows the crude and adjusted effect of predictors or risk factors for abdominal obesity. After adjusting for variables of Block I, being in the second year (odds ratio [OR] = 0.41; 95% CI: 0.19-0.88) and third year (OR = 0.18; 95% CI: 0.06-0.59) of high school was found to be a protective factor against abdominal obesity. None of the variables of Block II was associated with abdominal obesity in the adjusted model. After adjustment, adolescents presenting poor aerobic fitness had a 4.10 times higher probability (95% CI: 1.62-10.4) of abdominal obesity. Excess weight was a very strong risk factor for abdominal obesity (OR = 208.6; 95% CI: 47.7-911.7).
DISCUSSION
This school-based study was designed to investigate the distribution of different health outcomes among adolescents from public schools in Florianópolis, Santa Catarina, Brazil. A marked prevalence of abdominal obesity was observed among the adolescents studied and possible predictors of this metabolic risk were identified. These findings may contribute to the elaboration of collective health promotion programs aimed at combating and preventing central fat.
Fernandes et al. (5) investigated students from public and private schools in Presidente Prudente, São Paulo, using the same cut-off values as the present study and found that 14.8% of the adolescents had abdominal obesity. In a cross-sectional study involving adolescents from the southeast of Brazil, the prevalence of abdominal obesity was 15.4% (14). These prevalence rates are higher than those found in the present study, indicating that estimates of abdominal obesity differ between regions. This difference between regions was demonstrated in a study comparing the prevalence of central obesity between adolescents from the United States (34.7%) and South Korea (8.4%) (2). A study conducted in India on adolescents aged 12 to 17 yr reported a prevalence of abdominal obesity of 4% (3). The authors emphasized that, in addition to hereditary and lifestyle factors that might account for differences between regions, the lack of consensus regarding cut-off values for the prediction of abdominal obesity impairs comparisons between studies. This fact supports the need for investigations establishing predictors of abdominal obesity and specific cut-off values for each country.
The present study was consistent in demonstrating a higher prevalence of abdominal obesity among adolescents in the first year of high school, associated with low aerobic fitness and excess weight. No studies are available that include school grade as a variable associated with abdominal obesity. However, since school grade is a predictor of educational level, it might be associated with some health outcomes as observed for maternal and paternal educational level (5).
With respect to aerobic fitness, Janz et al. (15) investigated this parameter and metabolic components in children and adolescents over a period of 5 yr. The authors observed that good aerobic fitness reduces the risk of abdominal obesity by 15%, elevated total cholesterol levels by 11%, and elevated LDL-cholesterol levels by 5%. Supporting these findings, an experimental study investigating the effects of 16-week aerobic exercise interventions found that improved aerobic fitness reduced abdominal, subcutaneous and visceral fat (16). Thus, one of the strategies to reduce abdominal obesity and the risks associated with this condition is to encourage physical exercise that improves aerobic fitness.
Excess weight has been associated with abdominal obesity. Park et al. (2) investigated metabolic risk factors in North American and Asian adolescents. The authors reported a prevalence of abdominal obesity of 61.3% and 87.7% among overweight and obese adolescents from the United States, respectively, and of 26.4% and 64.9% among overweight and obese adolescents from South Korea. Fernandes et al. (5), analyzing family factors associated with abdominal obesity, observed that not only excess weight of the adolescents but also excess weight of the parents was associated with abdominal obesity. In this respect, strategies against abdominal obesity must include the combat and prevention of excess weight. In addition to the school that should provide guidance regarding the importance of a healthy lifestyle, including regular physical activity, improvement of aerobic fitness and healthy eating habits, the family may especially contribute to the combat of excess weight by encouraging and providing opportunities for these behaviors and by serving as a reference (5).
No association between abdominal obesity and physical activity was observed in the present study. In adolescents, this association is being investigated (17-19) but the results are not conclusive. Ortega et al. (17), studying the physical activity pattern of Swedish children and adolescents by accelerometry, found that subjects performing vigorous physical activity (> 6 METs) presented a smaller WC than those performing mild to moderate activities. Kelishadi et al. (18) observed no association between physical activity evaluated by a questionnaire and abdominal obesity in Iranian adolescents. According to Kim and Lee (19), these findings suggest two situations: 1) abdominal obesity is inversely associated with vigorous physical activity; 2) there is no association between abdominal obesity and physical activity level when the latter is investigated using a questionnaire. Questionnaires do not directly evaluate these activities and most of them do not distinguish between different types of physical activity (19).
With respect to eating habits, international studies indicate that excess consumption of certain types of foods is associated with abdominal obesity (20, 21). Studying Irish adults, McCarthy et al. (20) showed that subjects consuming 1 g/day additional red meat in the form of hamburgers, hot dogs and sausages and canned meat presented a 1% higher chance of developing abdominal obesity. An Italian cross-sectional study demonstrated that excess intake of total fat was positively associated with an increased WC, irrespective of gender (21). Brazilian studies investigating the association between the consumption of certain types of food and abdominal obesity are scarce. Therefore, studies performing a detailed analysis of the association between the type of food and central fat in Brazilian adolescents are necessary.
The cut-off values for abdominal obesity proposed by Taylor et al. (4) were developed for children and adolescents aged 3 to 19 yr from New Zealand. These values were chosen in the present study since there are no critical WC values for abdominal obesity developed for a sample of Brazilian adolescents. In addition, Taylor et al. (4) found a high sensitivity and specificity between WC cut-off values and trunk fat mass evaluated by DXA. Furthermore, previous studies involving adolescents from other Brazilian cities (5, 14) also used the cut-off values proposed by Taylor et al. (4), a fact permitting comparison between different Brazilian localities.
The main limitation of the present study is that no hereditary factors were analyzed as predictors of abdominal obesity in adolescents. An association between parental and childhood obesity has been reported in other studies (5). Another limitation was the lack of critical values for abdominal obesity developed for a sample of Brazilian adolescents. The use of the New Zealand cut-off values might have underestimated the prevalence of abdominal obesity because of its high frequency in that population (4).
The present school-based cross-sectional study and subsequent multivariate analysis of the data permitted to estimate the prevalence of abdominal obesity among adolescents and to identify associated factors. Knowledge about the distribution of abdominal obesity in the population contributes to the planning of more effective measures to reduce this public health problem. However, in order to propose effective actions, it is necessary to understand that, although factors associated with abdominal obesity such as level of aerobic fitness and nutritional status are considered to be modifiable, different levels of actions are used to reverse this situation. This study identified factors that require the dissemination of knowledge and specific actions addressing schoolchildren and, at the same time, distal factors in the determination chain such as school grade that require the restructuring of existing social policies in the country, especially those related to school and family.
In conclusion, demographic and lifestyle factors exert an impact on the quantity of abdominal fat. Factors such as school grade, low aerobic fitness and excess weight are associated with central obesity.



 XML Download
XML Download