

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
During the past years, earthquakes occurred here and there throughout the world. At 2:28 p.m. Beijing time on 12th May 2008, an earthquake registering 8.0 on the Richter scale devastated the mountainous region of Sichuan in China, and the epicenter was at Wenchuan County in Sichuan Province of China. In respect of losses of life, earthquake is the most harmful disaster among all kinds of natural disasters (1). In the Sichuan earthquake, 69,227 people were killed, 17,923 people were missing, and 374,643 people were injured due to building collapse and falling objects such as rocks (2). Among these people, some had sustained abdominal crush injury owing to the high-force impacts. Crush abdominal injury is associated with high rate of mortality in the aftermath of a catastrophic earthquake (3-6), which suggested that abdominal earthquake-related crush injury might be more severe due to its features different from non-earthquake injury. To prevent high rate of mortality in patients with abdominal earthquake-related crush injury, appropriate emergency therapies should be urgently performed shortly after the features of this crush injury have been better understood.
To illustrate the features of abdominal earthquake-related crush injury different from non-earthquake injury, multidetector computed tomography (MDCT) can be the reliable modality because CT scan of the abdomen could be considered as a gold standard for detecting intra- and retroperitoneal lesions in trauma patients (7, 8). To our knowledge, there were no reports regarding abdominal earthquake-related crush injury, and no publications to evaluate the features of abdominal earthquake-related crush injury different from non-earthquake injury by using CT (2, 9-11). Thus, the aim of our study was to retrospectively investigate the features of abdominal earthquake-related crush traumas in comparison with non-earthquake injury by pulling the names from a list of radiographic studies done during the similar periods in different years and then reviewing the records for better understanding and treating of patients with abdominal crush trauma in similar disasters in the future.
MATERIALS AND METHODS
Subjects
There were two groups in our study including the earthquake trauma and control group. Patients entered the present study as earthquake trauma group if they had blunt abdominal crush injury complicated with or without other system crush injuries such as injury in thorax and pelvis; if clinically suggested abdominal injury was initially confirmed by CT not greater than 14 days after the outbreak of this earthquake; and if the etiology of abdominal injury was crush injury in the 2008 Sichuan earthquake on the basis of the history and the findings of rescue. Patients were excluded from the earthquake trauma group if the etiology of the abdominal injury was not crush injury but jump or accidental fall from buildings, based on the history of injury in the earthquake. Patients with blunt abdominal trauma were enrolled into control group according to the inclusion criteria similar with those in earthquake trauma group except that the etiology was not associated with an earthquake.
In the 2008 Sichuan earthquake, an undamaged key university hospital 92 kilometers away from the epicenter, equipped with 4,300 beds, working as the largest-scale urgent care center in the earthquake-affected areas, received and treated a total of 2,728 victims with earthquake-related injury over a period of 14 days. Among these victims, 51 patients (22 men and 29 women; mean age, 41.9 yr; age range, 7-86 yr) with blunt abdominal crush injury in the Sichuan earthquake, who met the inclusion criteria, entered the present study as earthquake trauma group. In this group, 49 patients with abdominal crush injury were in combination with suggested crush injuries in one or more of other anatomic systems including the thorax, pelvis, extremity, and neck in 39, 40, 11, and 4 patients, respectively. In order to timely detect the injury for appropriate emergency treatments in a great number of injured patients as soon as possible, two of five MDCT scanners in this Department of Radiology were utilized to image the injury. The MDCT scans were followed with a routine renal function test and a measurement of the myoglobin in blood and urine shortly after the admission, and acute renal failure were confirmed in 36 patients in earthquake trauma group. The mean time from crush injury to the CT scans was 5.4 days with a range from 6 hr to 14 days. During the time from injury to rescue, few dangerously ill patients survived before being evacuated to this university hospital to receive effective treatments. Some of them had received antibiotics in disaster areas to prevent infection. Based on the image findings and clinical data, 37 patients with intra- or retroperitoneal injury, fracture of lumber vertebra, or sever injury of abdominal wall underwent surgical treatments; and the remaining patients received conservative treatments. The retro- or intraperitoneal injury and severer injury of abdominal wall in patients who had received surgical treatments were reconfirmed by the operative findings. Owing to the appropriate treatments, 49 patients were cured, and 2 died of crush injuries.
Between 1st May and 6th June 2009, 41 consecutive patients (27 men and 14 women; mean age, 34.5 yr; age range, 2-60 yr) with abdominal non-earthquake blunt injury, who were admitted in this key university hospital and met the inclusion criteria, were enrolled into the present study as the control group. In the control group, patients had abdominal injury due to traffic accidents (n = 12), assault (n = 10), falls (n = 8), work-related accidents (n = 5), crush injury (n = 4) and collision injury (n = 2). In the control group, 34 patients had abdominal injury in combination with suggested injuries in one or more of other anatomic systems including the pelvis (n = 21), thorax (n = 16), extremity (n = 5), neck (n = 6), maxillofacial region (n = 9), and head (n = 10). In this group, emergency MDCT scans were performed similarly with that in the earthquake trauma group, and followed by appropriate emergency treatments. The mean time from the injury to the CT scans was 4.6 days with a range from 0.5 hr to 12 days. Owing to timely and appropriate treatments, 40 patients were cured, and 1 died of the injury.
Computed tomography
In earthquake trauma group, 38 and 13 victims with abdominal crush injury underwent emergency scans with Philips Brilliance 16-section MDCT (Philips Healthcare, Eindhoven, Netherland) and Siemens Somatom Sensation 16-section MDCT (Siemens Medical Systems, Forchheim, Germany), respectively. Due to suspicion of acute renal failure in the massive earthquake, an emergency CT scan of abdomen was performed without intravenous contrast media from right diaphragmatic dome to pelvic basement as soon as possible. In the control group, all patients underwent similar non-enhanced emergency scans with Siemens Somatom Sensation 16-section MDCT. If the victims were suggested with other system injury, MDCT scans of the corresponding anatomic regions were performed along with scans of the abdomen to image all injuries. The scanning parameters used for both scanners were as follows: 120 kV, 250 mAs, gantry rotation time of 0.5 sec, pitch of 0.85, collimation of 16 × 0.75 mm, reconstructed section thickness of 5 mm, field of view of 380 mm, and matrix of 512 × 512 mm. If fractures of lumbar vertebrae were found, the reconstructed section thickness was 1 mm. Image data were transferred to a picture archiving communication system (Syngo-Imaging, Siemens Medical Solutions, Forchheim, Germany).
Image data analysis
Image data were retrospectively reviewed by two radiologists (with 12 yr and 11 yr of experience in radiology, respectively) working in consensus focusing on the detailed anatomic regions involved and types of the abdominal traumatic lesions, and injuries of other anatomic regions. The abdominal regions involved were classified as retroperitoneum, intraperitoneal space, lumbar vertebrae, and abdominal-wall soft tissue. The fractures of lumbar vertebrae were reviewed in detail by multiplanar reconstruction with a slab of 5-7 mm and three-dimensional reconstruction. So as to better understand overall types of abdominal injuries, traumatic lesions in abdominal parenchyma organ, peritoneal pathological changes (seroperitoneum and pneumoperitoneum), and injuries of abdominal aorta were reviewed. In order to better demonstrate severity of abdominal injury, combined injuries of other anatomic regions such as the thorax and pelvis were reviewed according to the traumatic lesions demonstrated in the published reports (10, 11).
Statistical analysis
Data analysis was performed with a statistical software package (version 13.0 for Windows, SPSS Inc., Chicago, IL, USA). To investigate the features of abdominal earthquake-related crush injury, we compared lumbar vertebral fractures, injury of abdominal-wall soft tissue, retroperitoneal injury, intraperitoneal injury, and injuries of other anatomic regions between earthquake trauma group and control group by chi-square tests. Comparison between retro- and intraperitoneal injury was performed by the similar test. A P value of less than 0.05 was considered significant.
RESULTS
Fractures of lumbar vertebrae and injury of abdominal-wall soft tissue
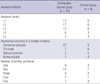
In earthquake trauma group, 24 of 51 patients (47.06%) had lumbar vertebral fractures (Fig. 1) in 49 vertebrae in comparison with 9 of 41 patients (21.95%) with the fractures in 25 vertebrae in control group. Lumbar vertebral fractures in earthquake trauma group occurred more frequently than in control group (P < 0.001). In groups, the fractures occurred in one or more vertebrae of L1-5 vertebra based on the anatomic levels involved. According to the structure of a lumbar vertebra involved, the fractures occurred in the transverse process, body, spinous process, or vertebral plate of the lumbar vertebra. Of these patients, the number of the lumbar vertebral fractures per patient ranged from 1 to 5. The involved vertebra levels, the structure, and the number of lumbar vertebrae are listed in Table 1.
Injuries of abdominal-wall soft tissue such as intramuscular hematoma, muscular swelling, fatty edema, or subcutaneous air collection were found in 54.9% patients (28/51) in earthquake trauma group, and in 31.7% patients (13/41) in control group. Injuries of abdominal-wall soft tissue were more common in earthquake trauma group than in control group (P = 0.019).
Retro- and intraperitoneal injury
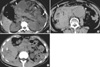
In earthquake trauma group, retroperitoneal injuries appeared as renal or perirenal injury, pancreatic injury, rupture of abdominal aortic aneurysm, swelling of perirenal fascia, and air collection in posterior perirenal space in 29 patients. In this group, renal or perirenal injuries appeared as hematoma, subcapsular hematoma, hemorrhage of renal cyst, and perirenal hematoma with or without swelling of perirenal fascia in 9 patients. Pancreatic injuries appeared as traumatic pancreatitis (Fig. 2A), or pancreatic rupture in combination with swelling of perirenal fascia in 3 patients. Renal injury in combination with pancreatic injury and abdominal aortic aneurysm (Fig. 2A, B) occurred in 1 patient, respectively. The remaining 15 patients in earthquake trauma group had swelling of perirenal fascia. In control group, 14 patients with retroperitoneal injuries manifested renal or perirenal injuries (n = 12), traumatic pancreatitis (n = 1), and renal injury in combination with traumatic pancreatitis (n = 1). Retroperitoneal injuries were more often seen in earthquake trauma group than in control group (P = 0.042).
Intraperitoneal injuries were found in 16 patients in earthquake trauma group, and were composed of liver injury in 7 patients, splenic injury in 2, hemoperitoneum in 5, and pneumoperitoneum in 2 (Fig. 2C). In control group, intraperitoneal injuries in 15 patients were composed of liver injury in 5 patients, splenic injury in 1, hemoperitoneum in 5, pneumoperitoneum in 3, and hydropneumoperitoneum in 1. In the two groups, incidences of intraperitoneal injuries were not different (P = 0.087). Retroperitoneal injury was more common than intraperitoneal trauma in earthquake trauma group (P = 0.008).
Abdominal injury in combination with injuries of other anatomic regions
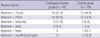
In earthquake trauma group, 43 patients had abdominal injury in combination with injuries of one or more other organs in the thorax (n = 29) and pelvis (n = 30). In control group, 29 patients had abdominal injury in combination with injuries of the thorax (n = 13) and pelvis (n = 15). The combined injuries of other organs are shown in Table 2. Abdominal injury in combination with injuries of other organs occurred more frequently in earthquake trauma group than in control group (P < 0.001).
DISCUSSION
Abdominal injury can result from both earthquake-related crush injury and non-earthquake injury (3-6, 12-15). As for earthquake-related crush injury, abdominal crush injury is associated with high rate of mortality, suggesting that abdominal earthquake-related crush injuries might be different from the non-earthquake injury due to high-force impact especially in the Sichuan earthquake registering 8.0 on the Richter scale (3-6). To better evaluate the difference of earthquake-related crush injury from non-earthquake injury, we performed this cohort study by using MDCT, and chose consecutive patients with abdominal non-earthquake injury presenting in the same university hospital during a similar period one year after the catastrophic earthquake as control group to reduce confounding factors of earthquake-related situation.
As shown in our study, both fractures of lumbar vertebrae and injury of abdominal-wall soft tissue occurred more frequently in patients with abdominal earthquake-related crush injury than with abdominal non-earthquake injury. According to the structure of a lumbar vertebra involved, fractures of transverse process were more common than of any other structure of a lumbar vertebra because the transverse process is one of the weakest parts of a lumbar vertebra. As reported by Dong et al. (10), most victims fell down and were trapped in prone posture when the earthquake occurred. When the high-force impact of falling objects stroke lower back, fracture of the transverse process might occur. In addition, the number of fractured lumbar vertebrae is a good indicator of severity of the injury. In the 2008 Sichuan earthquake, fractures of lumbar vertebrae occurred most frequently in one to two vertebrae. Regarding the vertebral levels involved, L1-3 fractures might be more common than any other vertebral levels involved in patients with abdominal earthquake-related crush injury, which was consistent with the previous report (9). Because high-force falling objects exerted impact to a comparatively wide region of posterior wall of the abdomen, multilevel fractures of lumbar vertebrae occur frequently.
Retroperitoneal injury occurred more frequently in patients with abdominal earthquake-related crush injury than with abdominal non-earthquake injury. However, intraperitoneal injury occurred in equal incidence in patients with either type of the abdominal injuries. These results can probably be attributed to the high-force impact of falling objects predominantly on lower back, which eventually results in retroperitoneal injury besides aforementioned fractures of lumbar vertebrae.
In retroperitoneal space, renal or perirenal injury might be more often seen than injuries of other retroperitoneal organs in an earthquake situation. According to Sever et al., the renal injury in the Marmara earthquake was vitally important since they could be directive for medical therapies as well as predict the final outcome (3). Therefore, it was necessary to timely diagnose renal injury from an earthquake for effective treatments to improve the therapeutic outcome.
In peritoneal cavity, liver injuries were more common than injuries of any other intraperitoneal organs. Full thickness bowel disruption was not represented in the patients with abdominal earthquake-related crush injury. The victims with these lethal injuries seem more often have died before the rescue was carried out. Thus, it is urgent to detect the abdominal injuries as early as possible for effective treatments in earthquake situation.
As illustrated in our study, abdominal injury in combination with injury of one or more of other organs could occur more frequently in patients with earthquake-related crush injury than with non-earthquake injury. The results suggested that abdominal earthquake-related crush injury could be more severe, and the injury in combination with that of other organs may be another good indicator in view of the severity of the abdominal injury because the combined injuries need more attention.
In the present study, low mortality of abdominal crush injury in the 2008 Sichuan earthquake could be found. According to Sever et al., abdominal injury was crush injuries associated with the higher mortality in the Marmara earthquake (3). Therefore, we could presume that most of severely ill patients with abdominal crush injury might have died prior to the rescue in the Sichuan earthquake. Owing to the death of the severe injured patients, most of them could not enter our study, which resulted in lowered mortality.
There was a limitation in this study. Contrast enhanced CT scan of abdomen could not be performed in the earthquake situation because acute renal failure was suggested by the crush syndrome, and iodinated contrast might potentiate the development of renal failure. Despite this limitation, the comparisons of earthquake-related crush abdominal injury with non-earthquake abdominal trauma could characterize the features of the crush abdominal injury in survivors. Our results may also be helpful in better understanding of the crush abdominal injury from other earthquakes for effective treatments of survived victims.
In conclusion, abdominal earthquake-related crush injury might be characteristic of high incidence in injury of abdominal-wall soft tissue, in fractures of lumbar vertebrae predominately in transverse process of one to two vertebrae among L1-3 vertebrae, in retroperitoneal injury predominately in kidney, and in combination with injury in other organs predominately in the thorax and pelvis. We expected that the features of abdominal crush injury could be helpful in proper diagnosis and treatment planning of the trauma patients in similar earthquakes in the future.

 XML Download
XML Download